Categories
Change Password!
Reset Password!


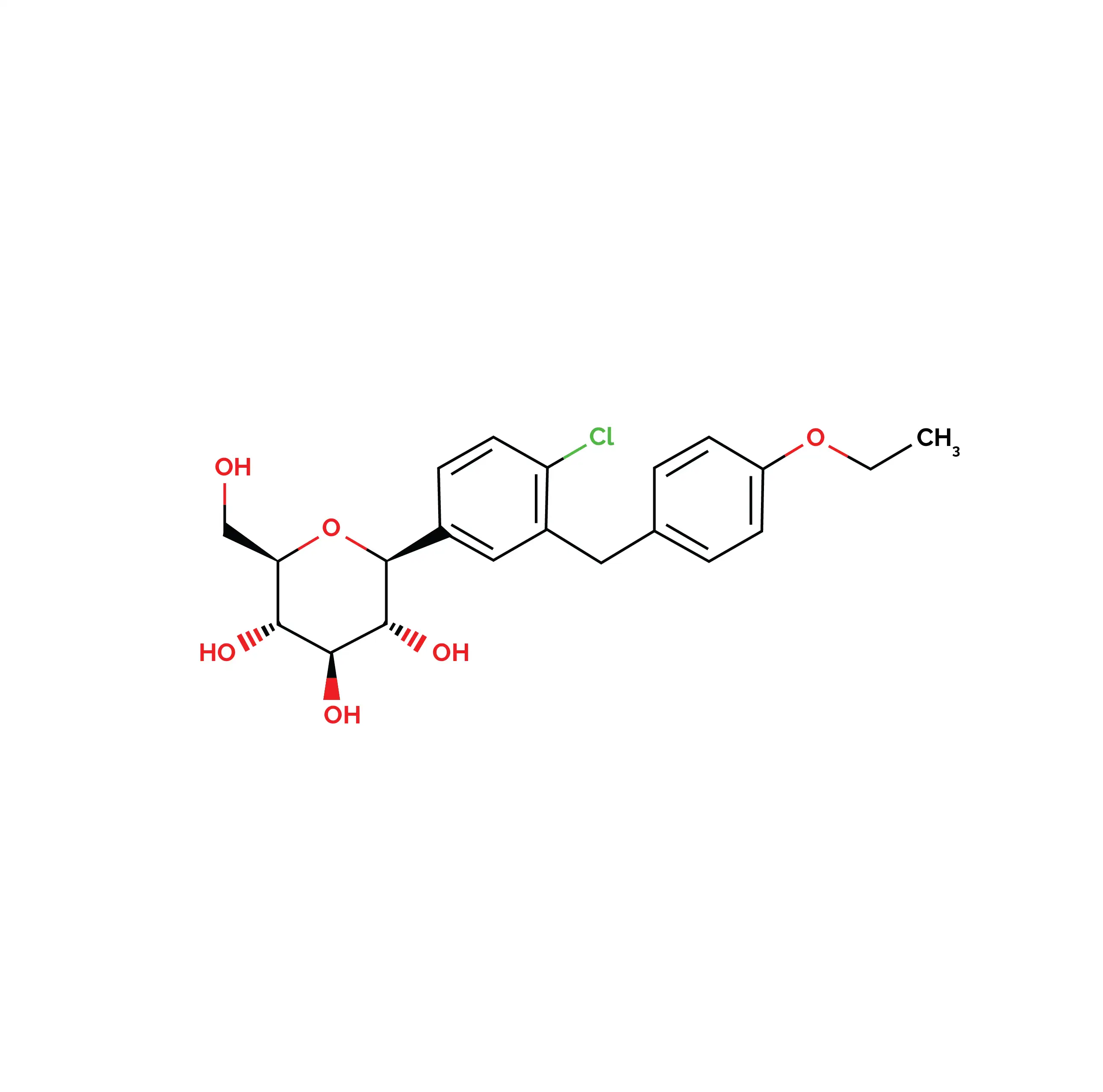
Dapagliflozin, an oral sodium-glucose cotransporter-2 (SGLT2) inhibitor, was first approved by the Food and Drug Administration (FDA) on January 8, 2014, for improving blood glucose control in type 2 diabetes mellitus (T2DM) when used alongside diet and exercise.
Dapagliflozin, an oral sodium-glucose cotransporter-2 (SGLT2) inhibitor, was first approved by the Food and Drug Administration (FDA) on January 8, 2014, for improving blood glucose control in type 2 diabetes mellitus (T2DM) when used alongside diet and exercise. In April 2021, its indications were expanded to include reducing the risk of worsening kidney disease, kidney failure, cardiovascular (CV) death, and hospitalization due to heart failure (HF) in chronic kidney disease.[1,2]
It works by blocking glucose reabsorption in the proximal renal tubules, leading to increased urinary glucose excretion along with mild weight loss and reduced blood pressure.[3]
Pharmacological Class: SGLT2 inhibitor
Dapagliflozin selectively inhibits SGLT2, responsible for ~90% of renal glucose reabsorption in the proximal tubules. Suppression of SGLT2 increases urinary glucose excretion, thereby improving glycemic control independent of insulin and contributing to modest weight loss in T2DM.[4]
Absorption
Dapagliflozin is rapidly absorbed by oral administration, achieving peak plasma concentration (Cmax) within 1–2 hours under fasting conditions. Exposure parameters [Cmax and area under the curve (AUC)] increase proportionally across the therapeutic dose range.
Dapagliflozin's (10 mg) absolute oral bioavailability is approximately 78%. Administration with a high-fat meal may delay Tmaxby nearly 1 hour and reduce Cmax; however, overall systemic exposure AUC remains unaffected, allowing administration with or without food.
Distribution
It demonstrates a mean volume of distribution of approximately 118 L. Moreover, it is about 91% bound to plasma proteins, and this binding remains unchanged in patients with renal or hepatic impairment.
Metabolism
It undergoes extensive hepatic metabolism primarily through glucuronidation, forming the major inactive metabolite, dapagliflozin 3-O-glucuronide. Minor metabolites include glucuronidated, de-ethylated, and hydroxylated derivatives. Metabolism is predominantly mediated by UGT1A9, with additional involvement of multiple CYP and UGT enzyme pathways.
Elimination
Dapagliflozin and its metabolites are predominantly eliminated through the renal route. Following administration of a single 50 mg dose of radiolabeled dapagliflozin, approximately 75% of total radioactivity is recovered in urine and 21% in feces. Dapagliflozin exhibits a mean terminal plasma half-life of 12.9 hours, enabling convenient once-daily administration. The oral plasma clearance is 4.9 mL/min/kg, while its renal clearance is 5.6 mL/min.[1]
Certain side effects associated with dapagliflozin include:
1. Post-hoc Analysis of DECLARE–TIMI 58: Dapagliflozin and Hospitalization Outcomes
The DECLARE–TIMI 58 trial explored dapagliflozin's effect on hospitalizations in patients with T2DM and multiple risk factors. In this randomized controlled study, 17,160 subjects received either dapagliflozin 10 mg daily or a placebo. As found, dapagliflozin reduced hospitalizations over a median follow-up of 4.2 years.
First non-elective hospitalizations for any cause occurred in 32.4% of patients receiving dapagliflozin compared with 35.4% in the placebo group, corresponding to an 11% relative risk reduction (hazard ratio [HR] 0.89). Total hospitalizations, including recurrent admissions, were also reduced (relative risk 0.92).
The reduction in hospitalization risk was consistent in patients both with established atherosclerotic CV disease (HR 0.92) and without established disease (HR 0.87). Dapagliflozin particularly reduced hospitalizations related to renal and urinary disorders by 39% (HR 0.61), metabolic and nutritional disorders by 27% (HR 0.73), cardiac disorders by 9% (HR 0.91), musculoskeletal and connective tissue disorders by 19% (HR 0.81), and infections by 14% (HR 0.86).[5]
2. Dapagliflozin and Gender-Based Outcomes in T2DM
A prespecified analysis of the DECLARE–TIMI 58 trial assessed whether the effects of dapagliflozin differed between women and men with T2DM. The study included 17,160 volunteers followed for a median of 4.2 years. Women accounted for 37.4% of the population and generallyhad higher glycated hemoglobin (HbA1c) levels, longer disease duration, and fewer background glucose-lowering therapies at baseline.
Dapagliflozin illustrated similar CV and renal benefits in both sexes. The drug reduced the risk of CV death or hospitalization for HF, while rates of major adverse CV events were comparable between dapagliflozin and placebo groups in both women and men. Renal outcomes also improved consistently, with reduced progression of kidney disease irrespective of gender.
The safety profile of dapagliflozin was comparable in women and men, with no prominent sex-related differences in adverse effects. Overall, the findings suggest that dapagliflozin provides consistent CV, renal, and safety benefits across both sexes in T2DM.[6]
1. Dapagliflozin. Drug Bank [DB06292]. Available from: https://go.drugbank.com/drugs/DB06292
2. Dapagliflozin. PubChem [9887712]. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Dapagliflozin
3. Padda IS, Mahtani AU, Parmar M. Sodium-Glucose Transport 2 (SGLT2) Inhibitors. [Updated 2025 Sep 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK576405/. Bookshelf ID: NBK576405, PMID:35015430.
4. FARXIGA® (dapagliflozin) tablets. FDA Label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/202293s020lbl.pdf
5. Schechter M, Wiviott SD, Raz I, Goodrich EL, Rozenberg A, Yanuv I et al. Effects of dapagliflozin on hospitalisations in people with type 2 diabetes: post-hoc analyses of the DECLARE-TIMI 58 trial. The Lancet Diabetes & Endocrinology. 2023 Apr 1;11(4):233-41.
6. O'Donoghue ML, Kato ET, Mosenzon O, Murphy SA, Cahn A, Herrera M et al. The efficacy and safety of dapagliflozin in women and men with type 2 diabetes mellitus. Diabetologia. 2021 Jun;64(6):1226-1234.













Comments (0)