Categories
Change Password!
Reset Password!



Fidaxomicin is a novel macrocyclic macrolide antibiotic and the first member of a new class of antimicrobial agents.
Fidaxomicin is a novel macrocyclic macrolide antibiotic and the first member of a new class of antimicrobial agents.[1,2] Approved by the Food and Drug Administration (FDA) in 2011, fidaxomicin is available as oral tablets and oral suspension to treat Clostridioides difficile (C. difficile)–associated diarrhea in adults and pediatrics aged ≥6 months.[3,4]
The drug is produced through fermentation of the actinomycete Dactylosporangium aurantiacum and functions as a locally active, bactericidal agent in the gastrointestinal tract. Due to its minimal systemic absorption, fidaxomicin achieves high intestinal concentrations while limiting systemic exposure, making it unsuitable for systemic infections. Its targeted activity against C. difficile and restricted use for confirmed or strongly suspected infections also helps reduce the development of antimicrobial resistance.[5]
Pharmacological Class: Macrocyclic antibiotic
C. difficile infection (CDI) is a gastrointestinal infection caused by the Gram-positive bacterium C. difficile, often occurring after antibiotic use disrupts normal gut flora, leading to bacterial overgrowth. The infection can range from mild antibiotic-associated diarrhea to severe, life-threatening complications.
After oral administration, fidaxomicin is converted into its active metabolite, OP-1118. Both fidaxomicin and OP-1118 exert bactericidal activity against C. difficile by selectively suppressing bacterial RNA polymerase during the initiation stage of transcription. RNA polymerase is a vital bacterial enzyme responsible for gene expression and several cellular processes essential for bacterial survival. During transcription initiation, the RNA polymerase core enzyme interacts with a sigma (σ) factor to recognize promoter regions on bacterial DNA and begin RNA synthesis.
Fidaxomicin interferes with this process by binding to the DNA–RNA polymerase complex and blocking the separation of DNA strands required for transcription initiation, ultimately suppressing messenger RNA synthesis. Its selective mechanism of action and unique binding site are believed to contribute to its narrow antimicrobial spectrum.[3]
1. Adult Dose
2. Pediatric Dose (6 Months to <18 Years)
(a) Tablets
(b) Oral Suspension (Weight-Based Dosing)
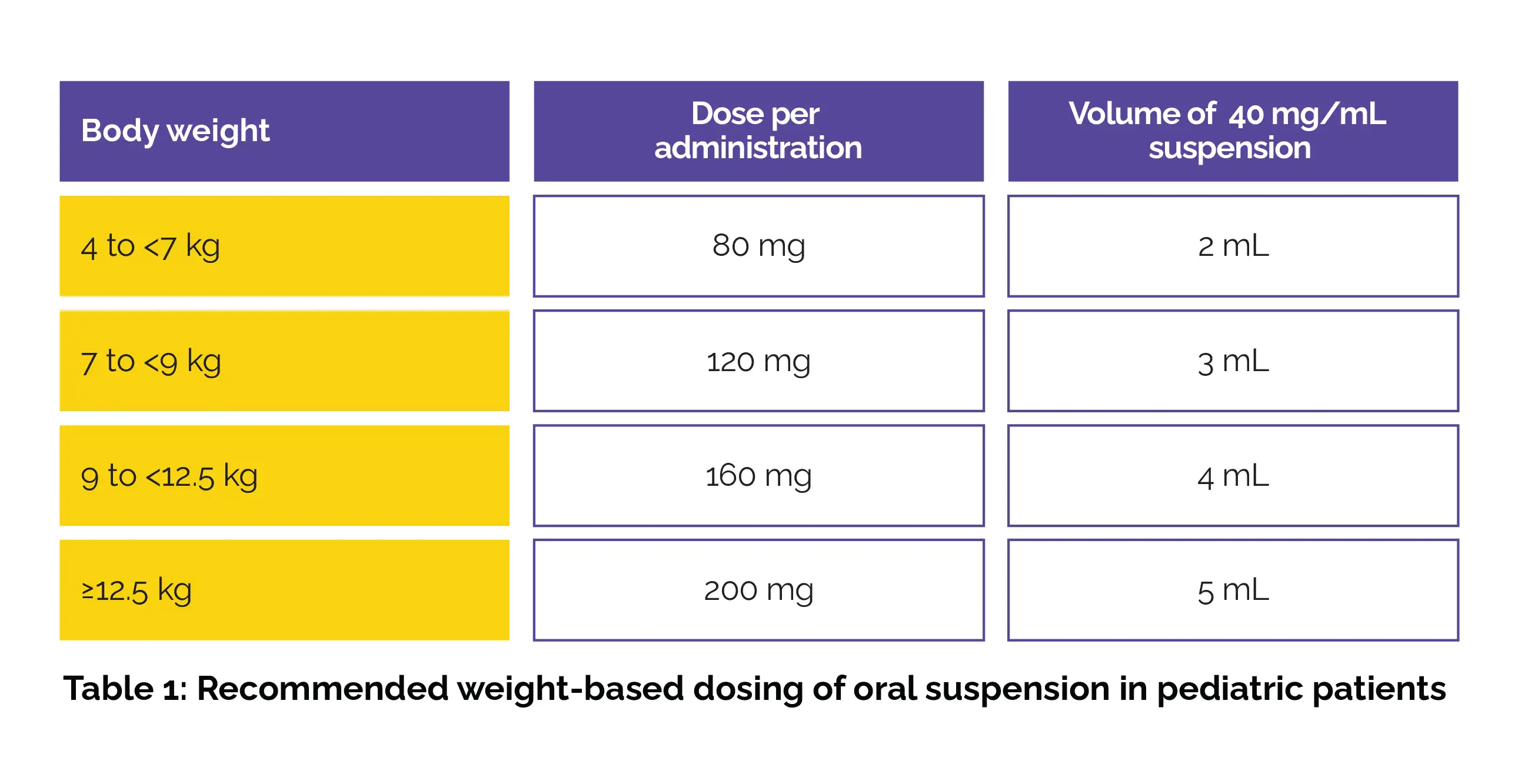
Notes
Absorption
Following oral administration of a single 200 mg dose in healthy adults, the mean maximum plasma concentration (Cmax) of fidaxomicin was 5.20 ± 2.81 ng/mL, while that of its main metabolite OP-1118 was 12.0 ± 6.06 ng/mL. The median time to reach peak concentration (Tmax) for fidaxomicin was 2 hours. Systemic absorption after oral administration is minimal.
Administration with a high-fat meal reduced the Cmax of fidaxomicin and OP-1118 by 21.5% and 33.4%, respectively in a food-effect study. This reduction is considered clinically insignificant, as the therapeutic activity of fidaxomicin does not rely on systemic drug exposure.
Volume of distribution
After oral administration, the drug remains largely restricted to the gastrointestinal tract. Limited data are available regarding its volume of distribution.
Protein binding
Due to minimal systemic absorption, there is paucity of information on fidaxomicin's plasma protein binding.
Metabolism
After oral administration, the drug undergoes hydrolysis at the isobutyryl ester to form its pharmacologically active metabolite, OP-1118. Cytochrome enzymes are not implicated in this process, and the conversion is believed to be triggered by gastric acid or enzymatic activity within intestinal microsomes.
Route of elimination
Fidaxomicin is primarily eliminated via feces following oral administration. Over 92% of the administered dose was excreted in feces as either parent drug or metabolites. Approximately 0.59% of an oral 200 mg dose was recovered in urine as OP-1118.
Half-life
The mean elimination half-life following a single oral 200 mg dose in healthy adults was approximately 11.7 ± 4.80 hours.
Clearance
Information regarding the clearance of fidaxomicin is limited.
Note: In pediatric patients, fidaxomicin demonstrates minimal systemic absorption following oral administration, similar to the pharmacokinetic profile observed in adults. Across all pediatric age groups, plasma concentrations remain low and within the nanogram-per-milliliter range at therapeutic doses. Mean (± standard deviation) plasma concentrations measured 1–5 hours after dosing were 39.41 ± 62.15 ng/mL for fidaxomicin and 116.64 ± 259.10 ng/mL for its active metabolite, OP-1118.[3]
Fidaxomicin must not be used in those with known hypersensitivity to fidaxomicin or to any of its ingredients.[4]
The gastrointestinal P-glycoprotein (P-gp) efflux transporter mediates the transport of fidaxomicin and its primary metabolite, OP-1118. Cyclosporine, an inhibitor of multiple transporters including P-gp, significantly increases plasma concentrations of fidaxomicin and OP-1118 when co-administered, although concentrations remain within the ng/mL range. Inhibition of P-gp may reduce concentrations of fidaxomicin and OP-1118 at the gastrointestinal site of action; however, concomitant use of P-gp inhibitors showed no attributable effect on safety or treatment outcomes in controlled clinical trials.
Based on available data, fidaxomicin may be co-administered with P-gp inhibitors, and no dose modification is advocated. Clinical drug–drug interaction studies demonstrated that fidaxomicin has minimal effect on intestinal P-gp transport and major cytochrome P450 (CYP) enzymes, including CYP3A4, CYP2C9, and CYP2C19. Co-administration with digoxin, midazolam, warfarin, or omeprazole did not result in clinically relevant pharmacokinetic alterations, indicating that dose adjustment is generally unnecessary when fidaxomicin is used alongside P-gp or CYP enzyme substrates.[4]
1. In adults, the most commonly reported adverse events (≥2%) include:
2. Among pediatric patients, the most commonly reported adverse events (≥5%) include:
1. Fidaxomicin for C. difficile–Associated Diarrhea Prevention: DEFLECT-1 Trial
Clinical evidence was generated from a randomized, double-blind, placebo-controlled, multicenter trial in 611 adult patients undergoing autologous or allogeneic hematopoietic stem cell transplantation (HSCT) and receiving fluoroquinolone prophylaxis. Participants received either oral fidaxomicin 200 mg once daily or a placebo for up to 40 days during transplantation and antimicrobial therapy.
The primary composite endpoint (“prophylaxis failure”) was comparable between the fidaxomicin and placebo groups (28.6% vs 30.8%), largely because many failures were unrelated to confirmed C. difficile–associated diarrhea. However, confirmed C. difficile–associated diarrhea occurred significantly less often with fidaxomicin than with placebo (Table 2).
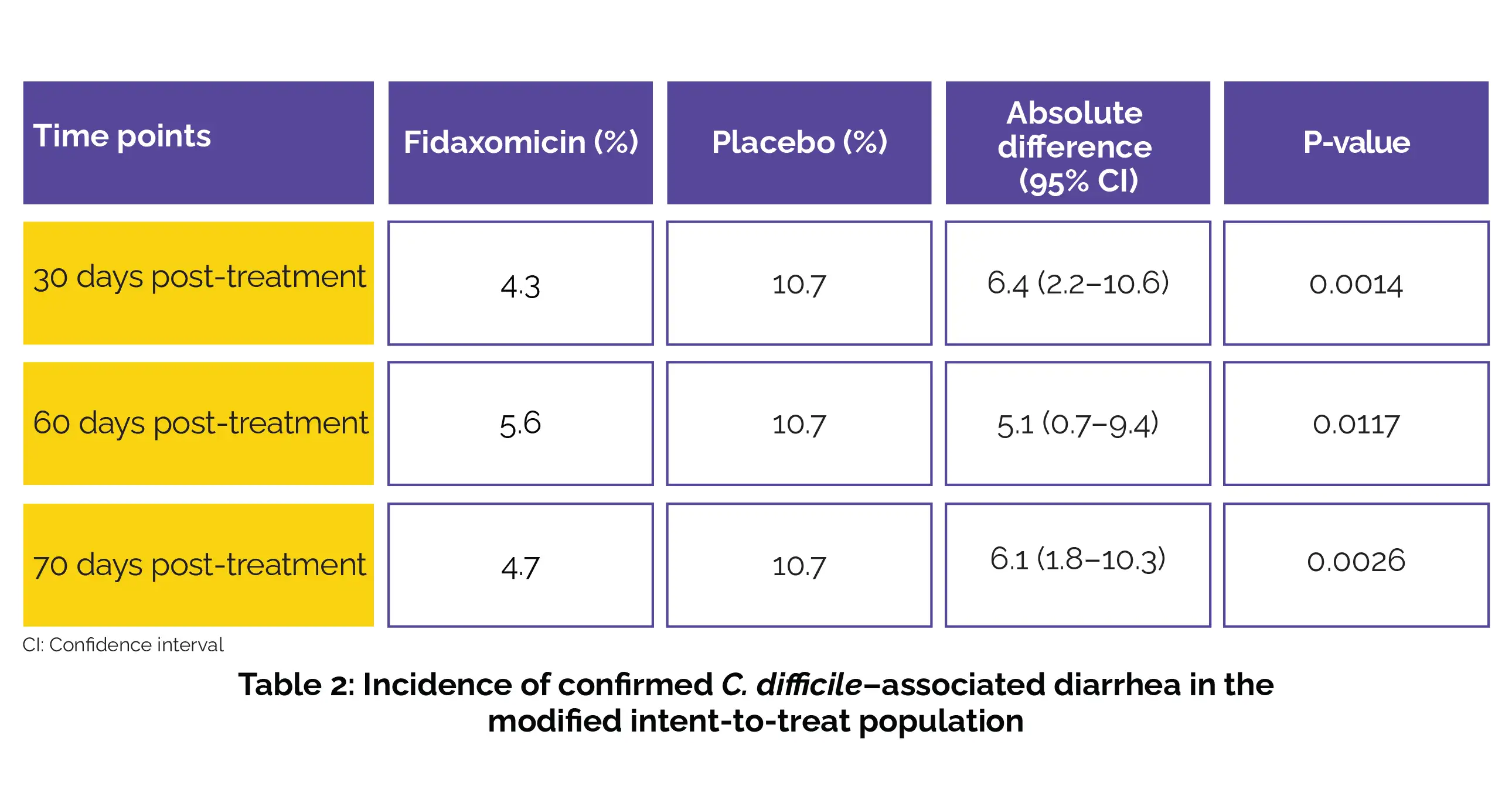
Treatment-related adverse events were also slightly lower in the fidaxomicin group (15.0% vs 20.0%). Although fidaxomicin did not considerably improve the composite primary endpoint, it markedly reduced the rate of confirmed C. difficile–associated diarrhea, supporting its potential role as prophylaxis in HSCT patients.[6]
2. Fidaxomicin vs. Vancomycin in CDI: Phase III Trials
Two multicenter, randomized, double-blind, vancomycin-controlled Phase III trials enrolled 1164 adults aged 18–94 years with diarrhoea and positive C. difficile toxin assay. Treatment consisted of fidaxomicin 200 mg every 12 hours or vancomycin 125 mg every six hours for 10 days, after which subjects were followed for 30 days.
Across both studies, per-protocol populations included 485 fidaxomicin-treated and 514 vancomycin-treated subjects, with representation of mild, moderate, and severe CDI.
Clinical cure rates were similar between groups (Table 3).

Sustained cure, defined as clinical cure without recurrence during follow-up, was higher with fidaxomicin due to lower recurrence rates. Adverse events were generally mild and occurred in fewer than 5% of patients. Overall, fidaxomicin was found to be non-inferior to vancomycin for initial cure while providing better protection against recurrence.[7]
3. Real-World Potency of Fidaxomicin in Preventing Recurrence of Community-Associated CDI
Clinical effectiveness was evaluated using population-based surveillance data from 1,193 adults with an initial episode of community-associated CDI in Monroe County, New York (2020–2024). Among included patients, 146 (12.2%) received fidaxomicin while 1,047 (87.8%) received vancomycin after completing an uninterrupted course of oral therapy.
The primary outcomes were CDI recurrence at 8 weeks and 90 days following initial intervention. Lower recurrence rates were observed with fidaxomicin compared with vancomycin (Table 4).
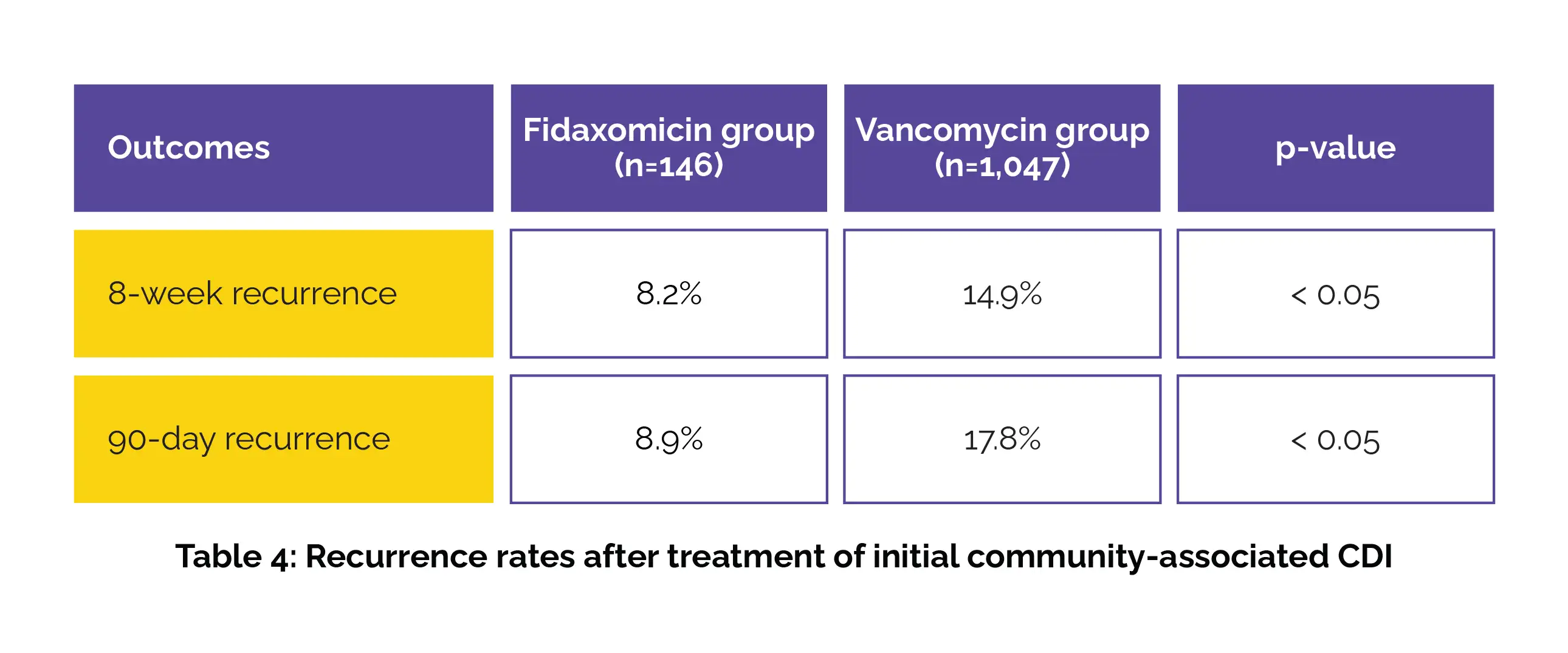
Crude analysis showed a higher risk of recurrence with vancomycin at 8 weeks (risk ratio [RR] 1.81; 95% CI 1.03–3.18) and 90 days (RR 2.00; 95% CI 1.17–3.41). After adjustment, vancomycin remained associated with increased recurrence at 90 days (RR 1.89; 95% CI 1.10–3.23). This real-world study demonstrates reduced recurrence with fidaxomicin compared with vancomycin in adults with initial community-associated CDI.[8]
4. Fidaxomicin vs. Vancomycin for CDI: A Propensity-Matched Real-World Analysis
Clinical outcomes were evaluated in a large real-world, propensity score–matched cohort comparing fidaxomicin and vancomycin as initial treatment for CDI. A total of 2,170 patients per group were included after matching, with comparable age and gender distribution. Fidaxomicin use was associated with lower event occurrence compared to vancomycin in 6 of 10 predefined clinical outcomes, including sepsis, candidiasis, death, and vancomycin-resistant enterococci (VRE) infection (Table 5).

Kaplan–Meier analysis demonstrated higher 12-month overall survival in the fidaxomicin group compared with vancomycin (87.06% vs. 78.49%, log-rank p < 0.001; hazard ratio 1.71). Fidaxomicin showed no survival difference versus vancomycin for surgical site infection, inflammatory bowel disease, and ventilator-associated pneumonia. For all other evaluated events, fidaxomicin was associated with superior survival outcomes.[9]
1. Mullane KM, Gorbach S. Fidaxomicin: first-in-class macrocyclic antibiotic. Expert review of anti-infective therapy. 2011 Jul 1;9(7):767-77.
2. Fidaxomicin. NIH. Pubchem [10034073]. Available from:
https://pubchem.ncbi.nlm.nih.gov/compound/Fidaxomicin
3. Fidaxomicin. Drugbank [DB08874]. Available from:
https://go.drugbank.com/drugs/DB08874
4. Fidaxomicin. FDA Label. Available from:
https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/213138lbl.pdf
5. Mullane KM, Gorbach S. Fidaxomicin: first-in-class macrocyclic antibiotic. Expert Review of Anti-infective Therapy. 2011 Jul;9(7):767-77.
6. Mullane KM, Winston DJ, Nooka A, Morris MI, Stiff P, Dugan MJ et al. A randomized, placebo-controlled trial of fidaxomicin for prophylaxis of Clostridium difficile–associated diarrhea in adults undergoing hematopoietic stem cell transplantation. Clinical Infectious Diseases. 2019 Jan 7;68(2):196-203.
7. Vaishnavi C. Fidaxomicin--the new drug for Clostridium difficile infection. Indian Journal of Medical Research . 2015 Apr;141(4):398-407.
8. Myers CJ, Hawco AJ, Dahhan R, Hurley C, van Wijngaarden E, Dumyati G. P-1005. Real-World Effectiveness of Fidaxomicin in Preventing Recurrence of Initial Community-Associated Clostridioides difficile Infection. InOpen Forum Infectious Diseases 2026 Jan (Vol. 13, No. Supplement_1, pp. ofaf695-1202). US: Oxford University Press.
9. Wingen-Heimann SM, Lübbert C, Bavaro DF, Hopff SM. Clostridioides difficile Infection in the United States of America-A Comparative Event Risk Analysis of Patients Treated with Fidaxomicin vs. Vancomycin Across 67 Large Healthcare Providers. Infectious Disease Reports. 2025 Jul 23;17(4):87.













Comments (0)