Categories
Change Password!
Reset Password!


Eravacycline is a fully synthetic fluorocycline antibiotic structurally related to tetracyclines. Approved by the Food and Drug Administration on 27 Aug 2018, this drug possesses broad-spectrum antibacterial activity against a wide range of Gram-positive, Gram-negative, anaerobic, and multidrug-resistant (MDR) organisms.
Eravacycline is a fully synthetic fluorocycline antibiotic structurally related to tetracyclines. Approved by the Food and Drug Administration on 27 Aug 2018, this drug possesses broad-spectrum antibacterial activity against a wide range of Gram-positive, Gram-negative, anaerobic, and multidrug-resistant (MDR) organisms. It is primarily used for the management of complicated intra-abdominal infections (cIAIs), especially in settings involving resistant pathogens such as:
It offers an important carbapenem-sparing option in antimicrobial stewardship programs.
Pharmacological Class: Tetracycline antibiotic[1]
It is used for cIAIs relief triggered by susceptible microorganisms, including Escherichia coli, Klebsiella pneumoniae, Citrobacter freundii, Enterobacter cloacae, Klebsiella oxytoca, Enterococcus faecalis, Enterococcus faecium, Staphylococcus aureus, the Streptococcus anginosus group, Clostridium perfringens, Bacteroides species, and Parabacteroides distasonis in adults aged 18 years and above.[2]
Eravacycline exerts its antibacterial effect by targeting the 30S ribosomal subunit, thereby blocking aminoacyl-tRNA attachment and disrupting bacterial protein synthesis. It generally exhibits bacteriostatic activity against Gram-positive organisms, including Enterococcus faecalis and Staphylococcus aureus. But, in vitro studies have illustrated bactericidal activity against select strains of Escherichia coli and Klebsiella pneumoniae.[1]
Absorption
Eravacycline exhibits dose-proportional pharmacokinetics, with increases in area under the curve and maximum drug concentration (Cmax) observed following single-dose IV administration across the dose range of 1 mg/kg to 3 mg/kg (up to three times the approved dose). Following repeated IV administration of 1 mg/kg every 12 hours, approximately 45% accumulation is observed at steady state.
Distribution
It demonstrates an extensive distribution profile, with a steady-state volume of distribution of approximately 321 L. Plasma protein binding is concentration-dependent, ranging from 79% to 90% across plasma concentrations of 100 to 10,000 ng/mL.
Metabolism
It is primarily metabolized through CYP3A4- and flavin-containing monooxygenase -mediated oxidative pathways.
Elimination
After administration of a single 60 mg IV dose of radiolabeled eravacycline, elimination occurs via both renal and fecal routes, with about 34% and 47% of the dose recovered in urine and feces, respectively. Excretion of unchanged eravacycline represents about 20% of the administered dose in urine and 17% in feces, with the remainder recovered as metabolites. The mean elimination half-life is nearly 20 hours with a clearance of 17.82 L/min.
Eravacycline should not be used in those with known hypersensitivity to eravacycline, other tetracycline-class antibacterial agents, or any component of the formulation.[2]
Common side effects
Other side effects
1. IGNITE 1 Trial
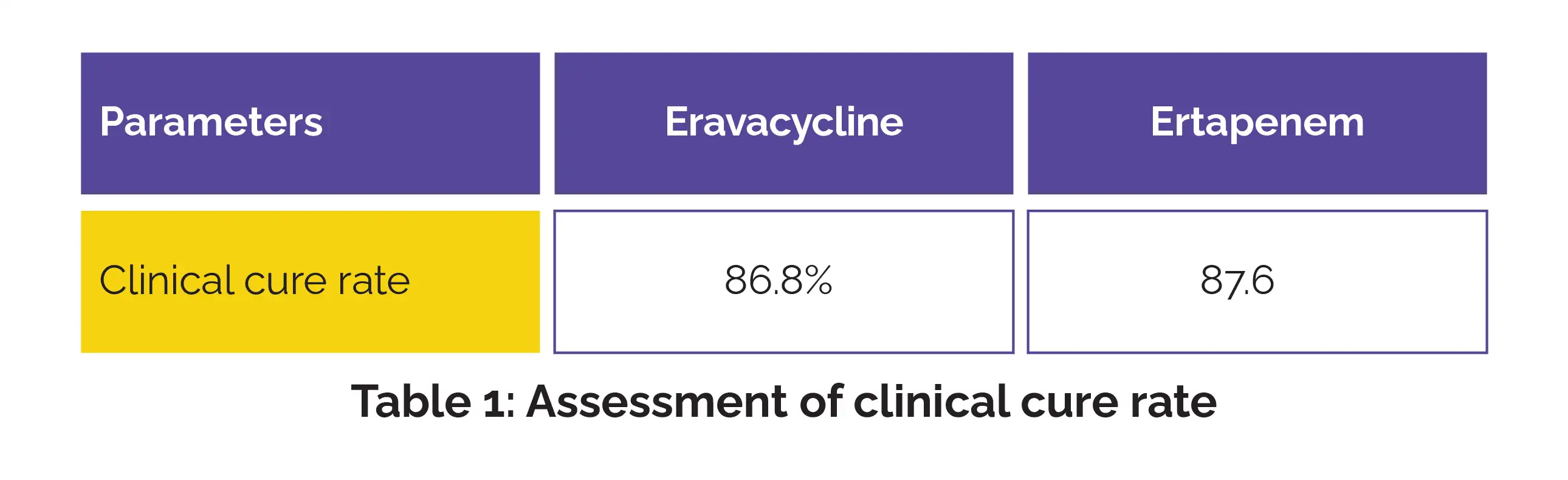
A phase III randomized study (IGNITE 1) evaluated eravacycline versus ertapenem in 541 hospitalized adults with cIAI needing surgical or percutaneous intervention. The test-of-cure assessment was performed 25–31 days after treatment initiation, while follow-up evaluations occurred 38–50 days after the first study drug dose.
Overall, 270 subjects (mean age 54.9 years) received eravacycline 1.0 mg/kg every 12 hours while 271 subjects (mean age 55.4 years) received ertapenem 1.0 g every 24 hours, for at least four 24-hour dosing cycles. Eravacycline demonstrated clinical outcomes comparable to ertapenem, achieving noninferiority with a favorable tolerability profile (Table 1).
Eravacycline showed consistent efficacy across common cIAI pathogens, including multidrug-resistant gram-negative organisms, while maintaining a tolerability profile similar to ertapenem. The study supports eravacycline as an effective, well-tolerated carbapenem-sparing treatment option for adult patients suffering from cIAI.[3]
2. IGNITE4 Trial
Another phase III randomized study (IGNITE 4) compared eravacycline with meropenem in hospitalized adults with cIAI. Patients received IV 1 mg/kg eravacycline every 12 hours or 1 g meropenem every 8 hours for 4–14 days. Eravacycline delivered clinical outcomes comparable to meropenem in cIAI, including infections caused by resistant gram-negative organisms (Table 2).
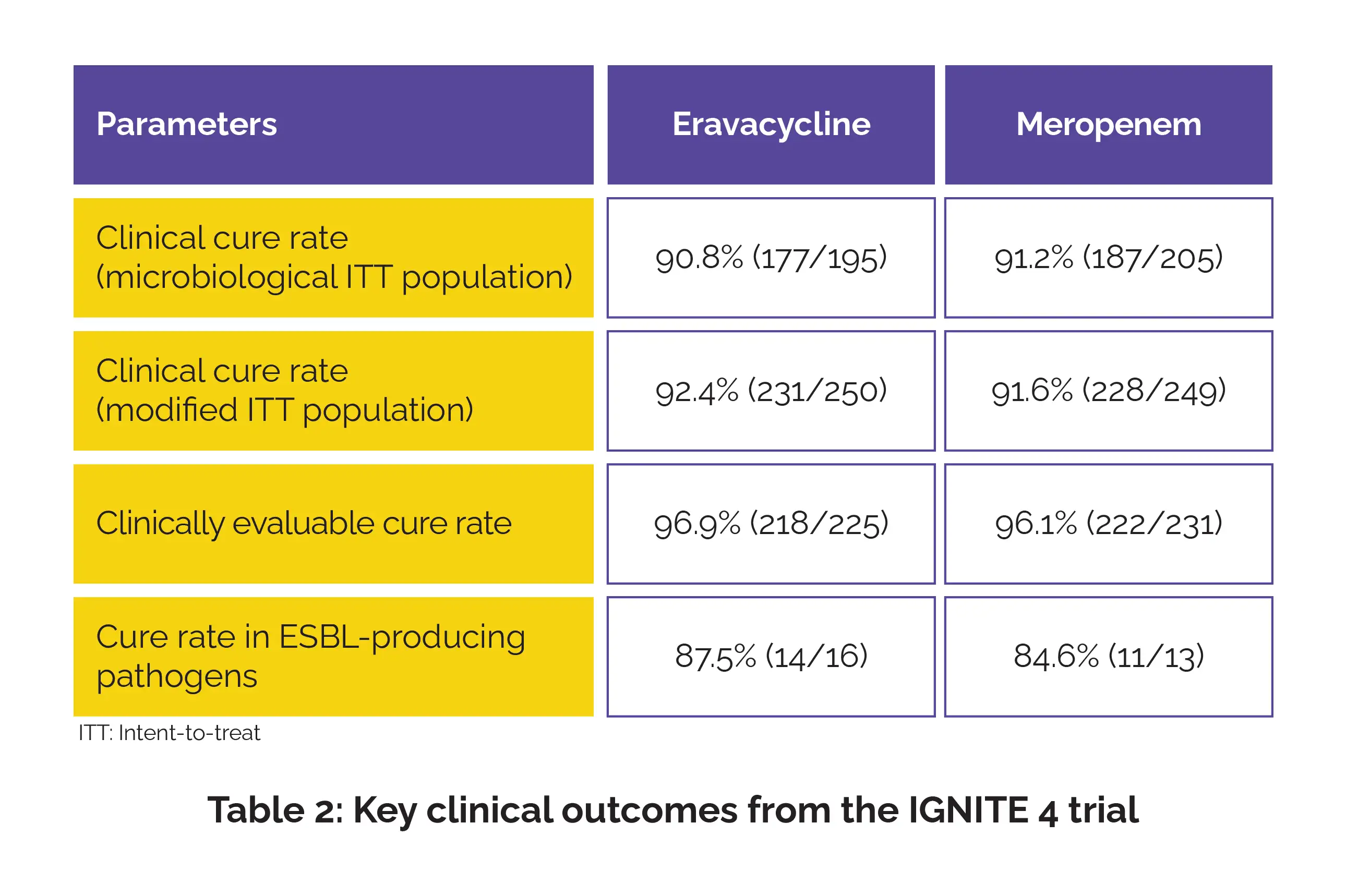
Eravacycline was generally well-tolerated, with low frequencies of gastrointestinal adverse events. Nausea, vomiting, and diarrhea were reported in fewer than 5%, 4%, and 3% of patients, respectively, supporting a favorable safety and tolerability profile.[4]
3. Systemic Review and Meta-Analysis of Randomized Controlled Trials (RCTs)
A pooled analysis of three RCTs assessed the efficacy and safety of eravacycline in adults with cIAIs. In the modified ITT population, the clinical cure rate at the test-of-cure visit was 88.7% (559/630) with eravacycline versus 90.1% (492/546) with comparator antibiotics (risk ratio [RR] 0.99). Comparable cure rates were also observed in the microbiological ITT (RR 0.99), clinically evaluable (RR 1.00), and microbiological evaluable populations (RR 0.98).
Clinical failure rates did not differ markedly between eravacycline and comparators across the modified ITT (RR 1.01), microbiological ITT (RR 1.34), clinically evaluable (RR 1.03), and microbiological evaluable populations (RR 1.32). Eravacycline also showed a safety profile broadly comparable to standard therapies.
While treatment-emergent adverse events were reported more frequently, serious adverse events, treatment discontinuation due to side effects, and all-cause mortality remained similar between treatment groups. These findings suggest that eravacycline offers efficacy comparable to standard therapies while maintaining an acceptable safety profile for cIAI treatment.[5]
4. Real-World Study
A recent single-center retrospective study evaluated real-world eravacycline use in 13 hospitalized patients with severe complicated infections, many involving highly resistant organisms. Most patients received combination therapy, predominantly with β-lactam antibiotics.
Clinical cure was achieved in 69.2% of patients, supporting eravacycline’s potential utility in difficult-to-treat MDR infections encountered in routine practice. Mortality was mainly associated with severe underlying illness, inadequate source control, and resistant pathogens.
Eravacycline was generally well-tolerated, with only one suspected case of drug-related hepatotoxicity reported. Although limited by its small sample size and retrospective design, the study adds supportive real-world evidence for eravacycline as a valuable option in complex MDR infections beyond cIAI.[6]
Eravacycline. Drugbank. Available from: https://go.drugbank.com/drugs/DB12329
2. Eravacycline. FDA Label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/211109lbl.pdf
3. Solomkin J, Evans D, Slepavicius A, Lee P, Marsh A, Tsai L. et al. Assessing the Efficacy and Safety of Eravacycline vs Ertapenem in Complicated Intra-abdominal Infections in the Investigating Gram-Negative Infections Treated With Eravacycline (IGNITE 1) Trial: A Randomized Clinical Trial. JAMA Surgery. 2017 Mar 1;152(3):224-232.
4. Solomkin JS, Gardovskis J, Lawrence K, Montravers P, Sway A, Evans D.et al. IGNITE4: Results of a Phase 3, Randomized, Multicenter, Prospective Trial of Eravacycline vs Meropenem in the Treatment of Complicated Intraabdominal Infections. Clinical Infectious Diseases. 2019 Aug 30;69(6):921-929.
5. Lan SH, Chang SP, Lai CC, Lu LC, Chao CM. The Efficacy and Safety of Eravacycline in the Treatment of Complicated Intra-Abdominal Infections: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine 2019 Jun 17;8(6):866.
6. Giuliano S, Martini L, Prataviera F, Moreal C, Flammini S, Terrosu G.et al. Eravacycline: Data Based on Real Evidence. NEW MICROBIOLOGICA. 2025 Jul;48(2):137-146.













Comments (0)