Categories
Change Password!
Reset Password!



Epidural analgesia (EA) is the most widely used method for labor pain relief, yet it is associated with epidural-related maternal fever (ERMF), which occurs in 15–25% of parturients.
Epidural analgesia (EA) is the most widely used method for labor pain relief, yet it is associated with epidural-related maternal fever (ERMF), which occurs in 15–25% of parturients. Maternal fever during labor has been related to prolonged hospital stays, postpartum hemorrhage, higher rates of cesarean section, and increased antibiotic use. Neonatal complications such as low muscle tone, early-onset seizures, lower Apgar scores, and a higher risk of infections have also been observed.
The pathophysiology involves sterile inflammation induced by local anesthetics, triggering cytokines (interleukin [IL]-1β, IL-6, IL-8), and prostaglandin-mediated thermogenesis. Prior interventions, such as steroids, have shown inconsistent benefits and potential neonatal risk. Kappa (κ)-opioid receptor agonists have anti-inflammatory properties and may mitigate fever via cytokine modulation. Butorphanol, a mixed κ-agonist/μ-antagonist, is widely used in labor analgesia and may offer a safe preventive strategy for ERMF.
Objective
This study aimed to evaluate whether intravenous (IV) low-dose butorphanol administered at the onset of EA could reduce the incidence of ERMF without compromising maternal or neonatal safety.
Sample size calculation
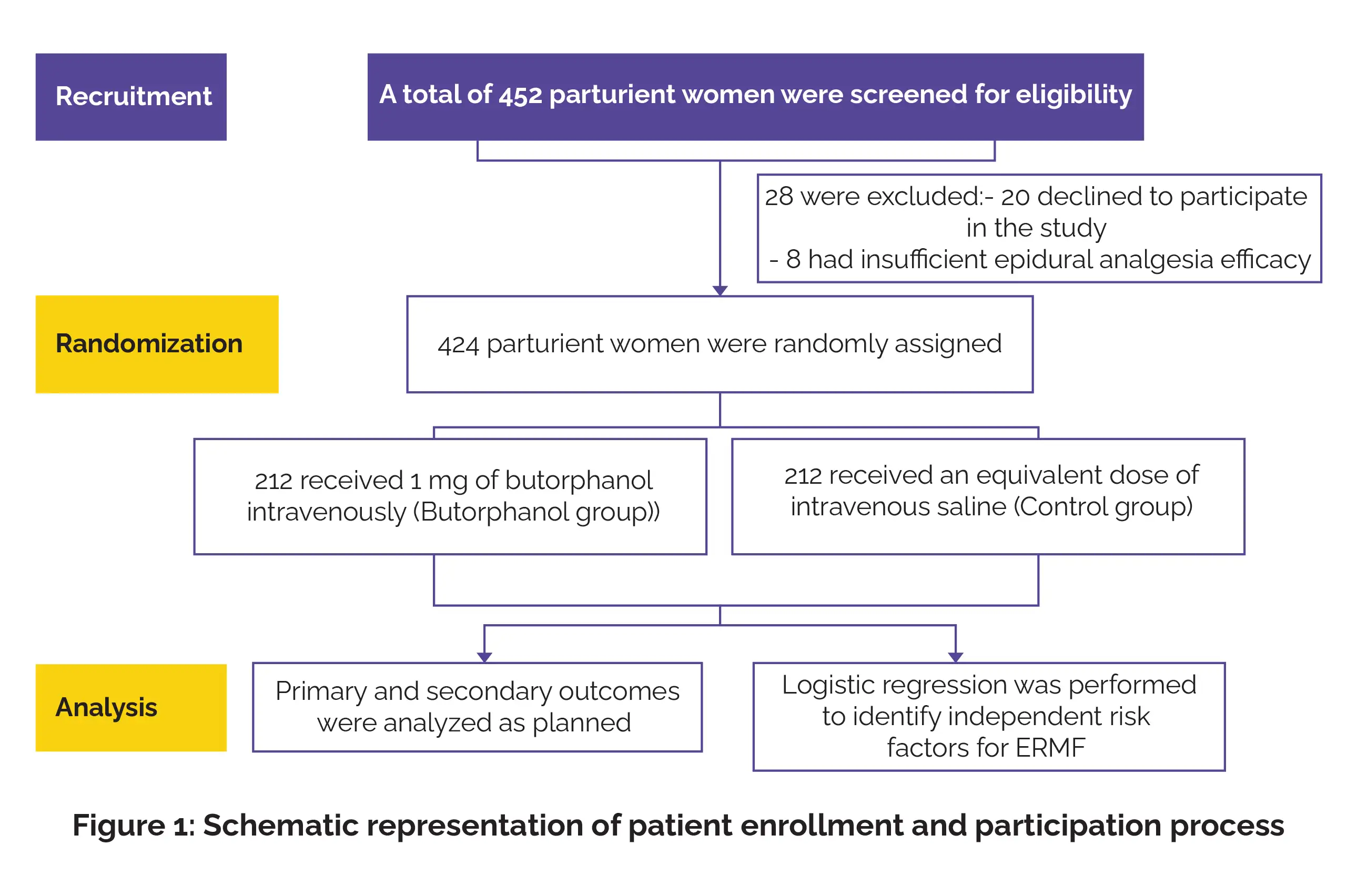
Retrospective data from the institution showed an intrapartum fever incidence of 15.2%. A pilot study of 30 participants suggested that prophylactic butorphanol could reduce this incidence by approximately 60%, with only 6.7% (2 cases) developing fever. Using a bilateral α = 0.05, power of 80% (1-β = 0.8), a 15% anticipated loss to follow-up, and a 1:1 allocation ratio, the required sample size was calculated as 212 participants per group (PASS 15.0).
Inclusion criteria
Exclusion criteria
Interventions
Eligible parturients were screened and, after confirming effective epidural analgesia (numerical rating scale [NRS] <4), were randomly assigned to two groups (n = 212 each):
In a delivery room maintained at 23°C, patients were monitored for blood pressure, heart rate, oxygen saturation, electrocardiogram, and fetal heart rate. Baseline systolic blood pressure (SBP) and heart rate were averaged from 3 readings between contractions. Phenylephrine (100 µg IV) was given if SBP dropped below 80% of baseline, and supplemental oxygen was provided if the saturation of peripheral oxygen (SpO2) fell below 95%. A 500 mL lactated Ringer’s infusion was started before analgesia.
Epidural analgesia was carried out in the left lateral position at the L2–L3 interspace using an 18G Tuohy needle, with catheter placement confirmed via loss-of-resistance technique. A test dose of 3 mL 1.5% lidocaine with epinephrine was administered to rule out intravascular or subarachnoid placement, followed by 10 mL of 0.125% ropivacaine with 0.4 µg/mL sufentanil. Patients achieving a pain score ≤3 at 30 minutes were randomized to receive either 1 mL saline or 1 mL butorphanol (1 mg/mL) IV.
Maintenance analgesia was provided via programmed intermittent epidural bolus (PIEB) of 0.08% ropivacaine with 0.4 µg/mL sufentanil, with 10 mL administered hourly. Patient-controlled epidural analgesia (PCEA) allowed 8 mL boluses with a 20-minute lockout, up to 35 mL/h, and additional 5–10 mL boluses could be administered manually if needed.
Outcome measures
1. Primary outcome
The primary outcome was the incidence of maternal fever related to EA. Axillary maternal temperature was measured hourly for the first 6 hours after EA initiation using a mercury thermometer. Fever was defined as a maximum temperature of ≥38°C, with secondary analysis at ≥37.5°C to capture low-grade fever.
2. Secondary outcomes
Secondary outcomes included maternal temperature, pain scores, total analgesic consumption, and delivery-related maternal and neonatal outcomes. Maternal outcomes included mode of delivery (vaginal, cesarean, or operative vaginal), labor duration, use of oxytocin or other uterotonic agents, and postpartum hemorrhage. Fetal outcomes comprised abnormalities in fetal heart rate (<110 or >160 beats/min), neonatal Apgar scores, and admission to the neonatal intensive care unit (NICU).
Statistical analysis
Continuous variables were examined via t-tests or Mann–Whitney U tests based on distribution. Categorical variables were explored with chi-square or Fisher’s exact test. Logistic regression detected independent predictors of ERMF. Odds ratios, risk ratios, and 95% confidence intervals were reported. P<0.05 was deemed significant.
Maternal temperature trend: Butorphanol exerted a protective effect by reducing the sustained rise in maternal temperature from the 2nd to the 5th hour after epidural analgesia (P < 0.05).
Pain control and analgesic use: No pivotal differences were observed in maternal pain scores or total analgesic consumption between groups (P > 0.05).
Adverse effects: Mild dizziness related to butorphanol occurred in a small number of participants within the first 2 hours after epidural analgesia (P < 0.05).
Safety outcomes: No severe maternal or neonatal adverse events were noted in either group.
This trial shows that butorphanol significantly reduces the incidence of both moderate (≥37.5°C) and high-grade (≥38°C) maternal fever associated with epidural analgesia. The butorphanol group demonstrated markedly lower fever rates, supporting the hypothesis that butorphanol attenuates the sterile inflammatory response associated with labor epidurals. Maternal temperature trajectories further confirm the drug’s effect, with significantly lower temperatures between 2 and 5 hours after analgesia compared with controls.
Analgesic efficacy remained preserved, as evidenced by similar NRS scores and comparable epidural drug consumption. Although the first stage of labor was slightly longer among women receiving butorphanol, overall obstetric outcomes—including mode of delivery, oxytocin use, and postpartum bleeding—remained similar. Neonatal outcomes demonstrated no adverse impact, with comparable Apgar scores, fetal heart rate patterns, and NICU admissions. Mild dizziness was more common early in labor in the butorphanol group, but no severe maternal or neonatal adverse effects were witnessed.
These findings align with the known anti-inflammatory properties of κ-opioid receptor agonists and suggest that butorphanol interrupts the cytokine-mediated pathways responsible for ERMF. Given the maternal and neonatal consequences of intrapartum fever, butorphanol represents a promising, safe, and easily implementable preventive intervention.
Butorphanol administered intravenously at the onset of EA significantly reduced both high-grade and low-grade maternal fever. Analgesic efficacy, labor progression, and neonatal outcomes remained unaffected. The only notable adverse event was mild transient dizziness within the first 2 hours. These findings support butorphanol as a safe and effective intervention to prevent ERMF and improve maternal and neonatal safety during labor.
Drug Design, Development and Therapy
Efficacy of Intravenous Butorphanol for Preventing Epidural-Related Maternal Fever (ERMF) During Epidural Labor Analgesia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial
Yao Zhang et al.













Comments (0)