Categories
Change Password!
Reset Password!



The relationship between obesity phenotypes and non-communicable diseases—including type 2 diabetes, hypertension, chronic kidney disease, cardiovascular disease, and cancer—is well established.
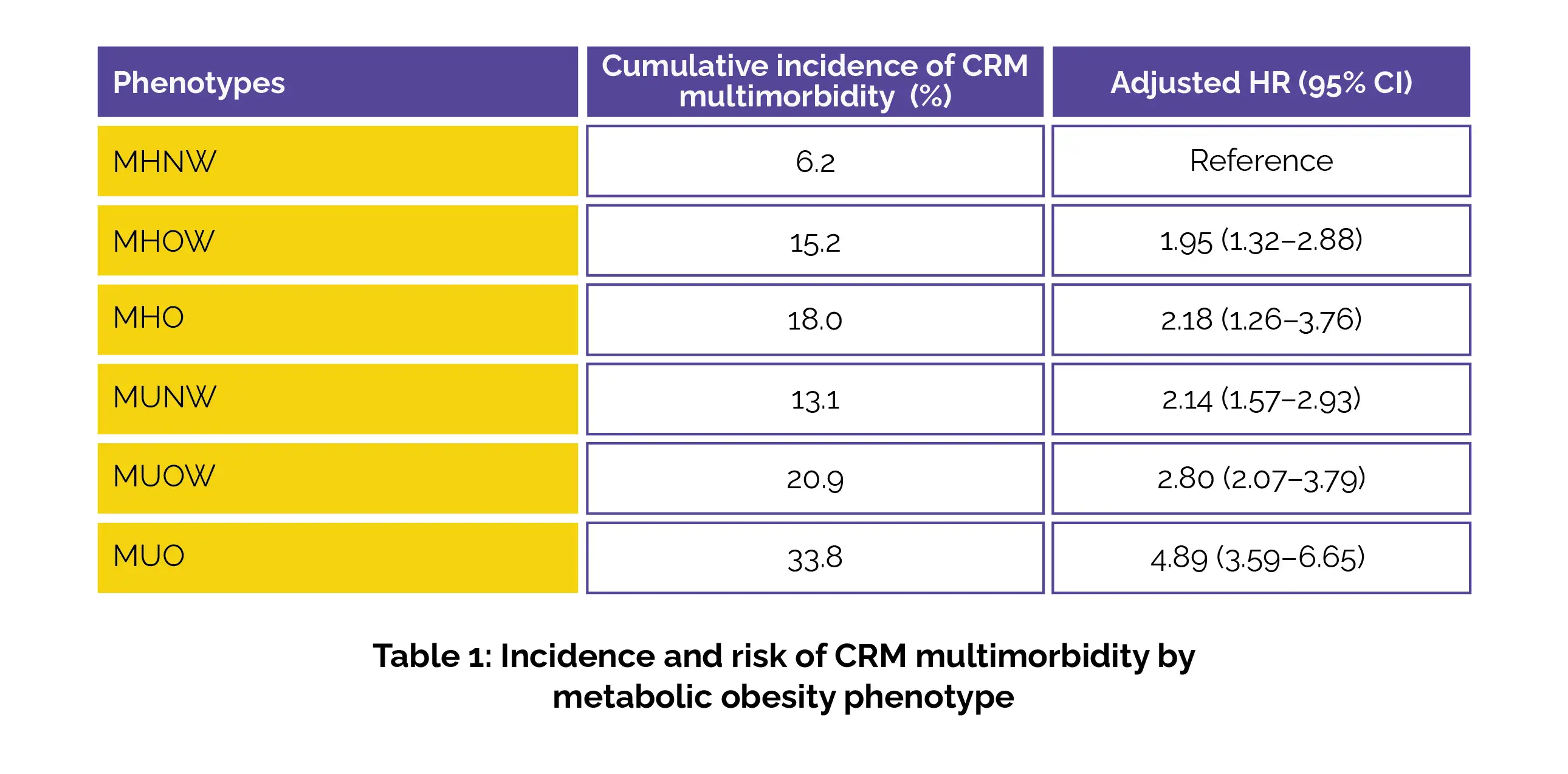
Metabolically unhealthy obese people exhibit the highest risk of developing cardio-renal-metabolic multimorbidity, with nearly a 5-fold increase compared to metabolically healthy normal-weight people.
The relationship between obesity phenotypes and non-communicable diseases—including type 2 diabetes, hypertension, chronic kidney disease, cardiovascular disease, and cancer—is well established. However, limited evidence exists regarding how different metabolic obesity phenotypes influence the likelihood of developing cardio-renal-metabolic (CRM) multimorbidity, defined as the coexistence of two or more major chronic conditions.
This study examined the long-term link between general obesity (based on body mass index, BMI) and central obesity (based on waist circumference) metabolic phenotypes with the incidence of CRM multimorbidity over nearly 2 decades in adults aged ≥20 years.
This prospective cohort study included 6,407 adults (3,588 women; mean age 37.1 years). Metabolically healthy status was described as the absence of metabolic syndrome components. Subjects were categorized as:
1. BMI-based phenotypes:
2. Waist circumference-based phenotypes:
For assessing hazard ratios (HRs) and 95% confidence intervals (CIs), multivariable cox proportional hazards regression models were applied.
During a median follow-up of 14.3 years, the risk of CRM multimorbidity heightened progressively across adverse metabolic phenotypes. Compared with MHNW individuals, significantly higher risks of CRM multimorbidity were observed in the other counterparts (Table 1).
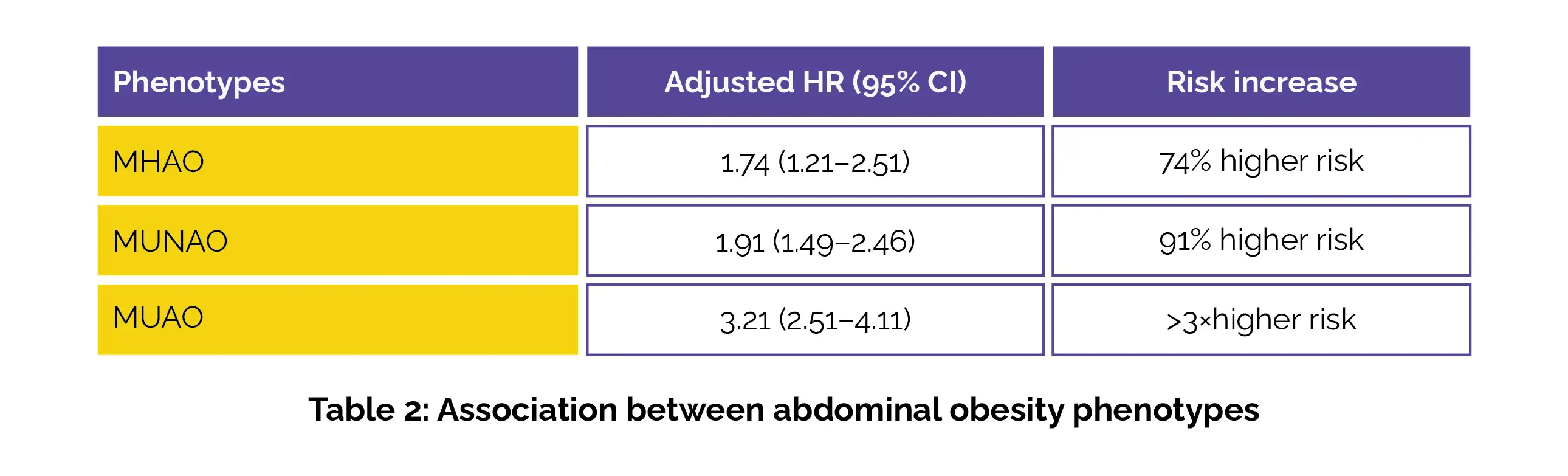
Using MHNAO as a reference, elevated risks were also found for MHAO, MUNAO, and MUAO (Table 2):
No statistically significant interaction by age or sex was detected. However, the links were more pronounced among women and younger adults, suggesting higher susceptibility in these subgroups.
Maintaining normal body weight combined with optimal metabolic health mitigates the long-term risk of CRM multimorbidity. Importantly, even individuals classified as MHO face increased risk over time, challenging the concept of “benign obesity”. These findings reinforce the importance of early obesity management, metabolic screening, lifestyle modification, cardiometabolic risk assessment, and preventive healthcare strategies.
European Heart Journal
Different metabolic phenotypes of obesity and two decades risk of cardio-renal-metabolic multimorbidity
D Molavizadeh et al.










Comments (0)