Categories
Change Password!
Reset Password!



Integrated clinical testing with MRI—especially nerve root sleeve angulation and lumbar lordosis—accurately differentiates discogenic ULLRP from sacroiliac joint dysfunction and piriformis syndrome in adults.
Unilateral lower limb radicular pain (ULLRP) is a complex condition that impairs mobility and daily activities. While lumbosacral disc issues are common, sacroiliac joint dysfunction and piriformis syndrome can produce similar symptoms, making accurate clinical-radiological correlation essential. This prospective analytical study examined clinical profiles, spinopelvic alignment, and magnetic resonance imaging (MRI) findings in adults with ULLRP, while examining the impact of lifestyle and occupational factors across diverse ethnic groups in Sikkim, India.
The study analyzed ambulatory adults over 18 with ULLRP, excluding those with bilateral symptoms, prior spine surgery, spinal deformities, hip-pelvic pathology, fractures, tumors, or imaging contraindications. Clinical evaluation included visual analog scale (VAS), straight-leg raise (SLR), sitting SLR, slump, FABER (flexion, abduction, and external rotation), FAIR (flexion, adduction, and internal rotation), femoral stretch, and motor, myotomal, and dermatomal evaluation.
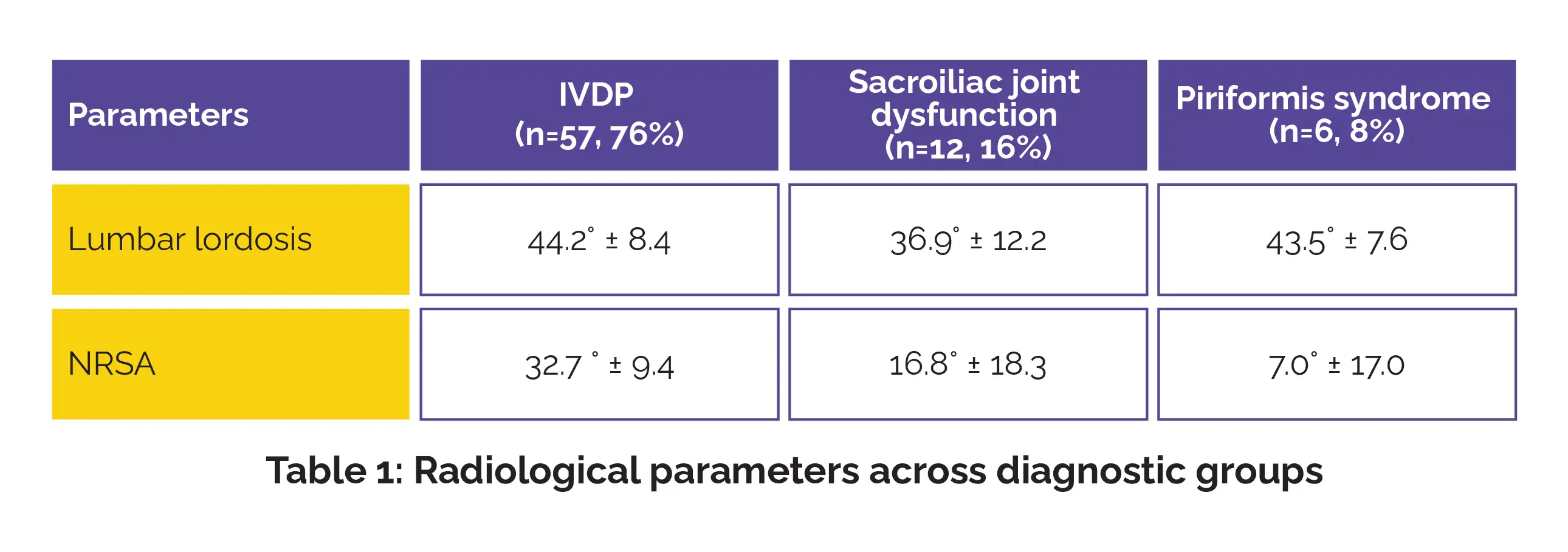
Standing lateral radiographs assessed pelvic incidence, pelvic tilt, sacral slope, and lumbar lordosis, while MRI (1.5T) evaluated nerve root sleeve angulation (NRSA) between affected and unaffected sides. Primary outcomes were clinical and radiologic profiles; secondary outcomes included lifestyle and occupational factors.
A total of 75 patients were analyzed (mean age 44.5 ± 12.5 years; 56% women), with a mean VAS score of 6.7 ± 1.4, indicating moderate-to-severe pain.
Key clinical correlations included:
Significant radiological distinctions were noted:
Lifestyle factors like ethnicity, smoking, alcohol intake, diet, and occupation showed descriptive variation but did not reach statistical significance. Integrating detailed clinical tests with MRI evaluation, including NRSA and lumbar alignment, markedly boosts diagnostic accuracy in ULLRP. While disc prolapse remains the most common cause, sacroiliac and piriformis syndromes are notable contributors. This structured clinical-radiological approach enables precise differentiation of causes, guiding targeted treatment and optimizing patient outcomes.
By integrating advanced MRI markers with meticulous clinical examination, clinicians can better differentiate discogenic from non-discogenic radicular pain. This refined approach may optimize patient triage, minimize unnecessary interventions, and support personalized conservative or targeted therapeutic strategies for adults with ULLRP.
International Journal of Pharmacy Research & Technology
Clinical and Radiological Correlates of Unilateral Lower Limb Radicular Pain: An Analytical Study (February 2025)
Singh AD et al.














Comments (0)