Categories
Change Password!
Reset Password!


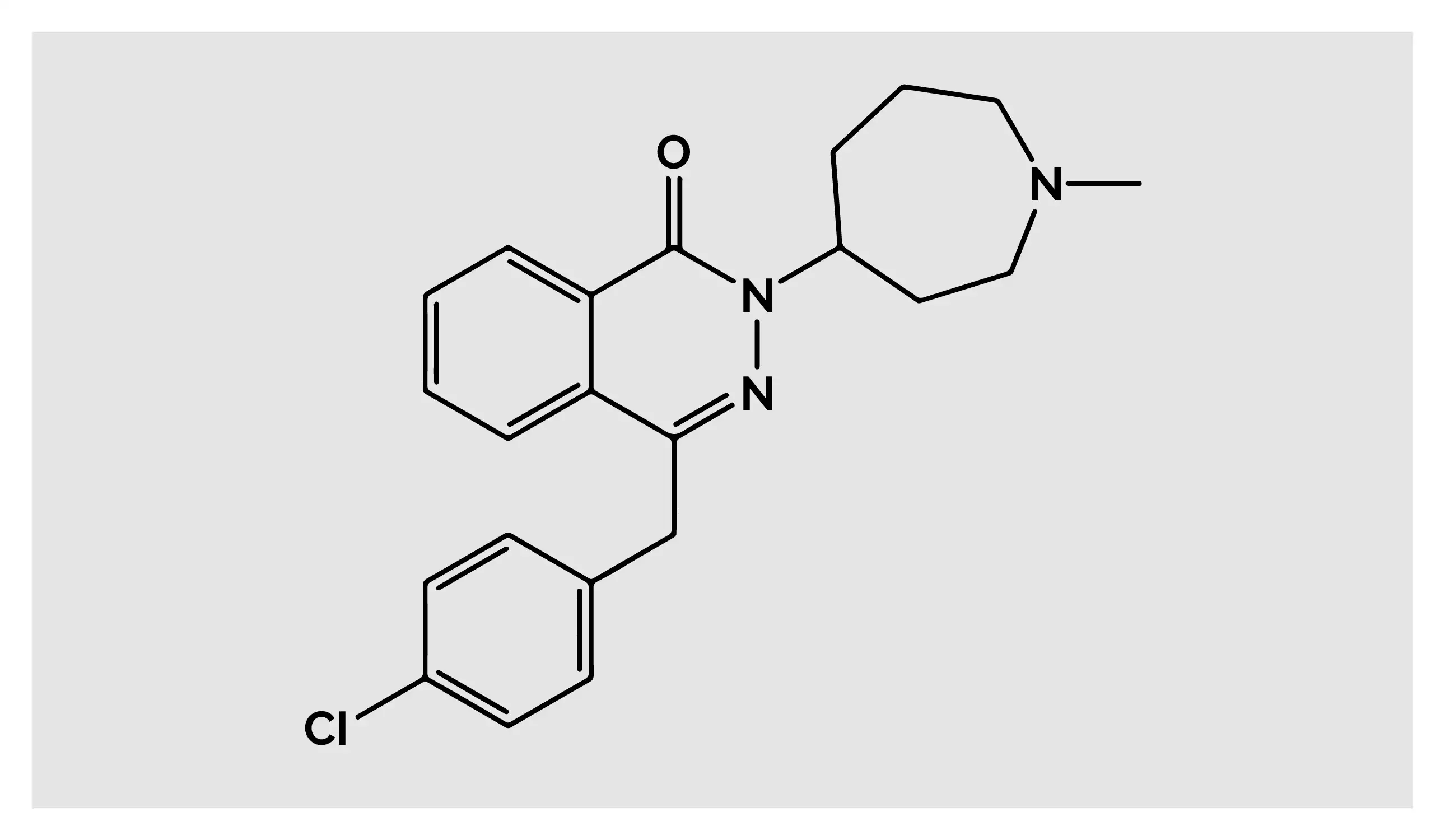
Azelastine, first granted approval in 1996, is a histamine H1-receptor antagonist used to treat allergic and vasomotor rhinitis, as well as allergic conjunctivitis.
Azelastine, first granted approval in 1996, is a histamine H1-receptor antagonist used to treat allergic and vasomotor rhinitis, as well as allergic conjunctivitis. [1] Owing to the broad spectrum of anti-inflammatory and anti-allergic activity, Azelastine can alleviate sneezing, nasal itching, runny nose, nasal congestion, and other symptoms.[2-4]
Pharmacological Class: Antihistamine [1]
Azelastine is indicated to treat symptoms of:
The phthalazine derivative Azelastine is principally a selective antagonist of histamine H1-receptors, with a reduced affinity for H2-receptors, and is used for symptomatic management of allergies. Histamine H1-receptors are present on glandular cells, smooth muscle cells, and nerve terminals. The immunoglobulin E-receptor (IgE-receptor) cross-linking on mast cells causes histamine to be produced following allergen exposure in persons with sensitization. Histamine binds to H1-receptors and triggers allergic symptoms (for example: congestion, sneezing, and itching).
Azelastine seems to influence other mediators of allergy symptomatology even though its key mechanism of action is assumed to be via H1-receptor antagonism. Azelastine has been reported to have mast cell-stabilizing activity that restricts release of interleukin-6, tryptase, histamine, and tumor necrosis factor (TNF)-alpha from mast cells. Furthermore, it lowers mediators of mast cell degranulation like leukotrienes in nasal lavage of people suffering from rhinitis. By suppressing phospholipase A2 and leukotriene C4 synthase, it prevents them from being produced and released by eosinophils. [1]
(a) Children between the ages of 5 and 11 years: Twice daily, one spray per nostril
(b) Adults and adolescents ≥12 years: 1 or 2 sprays twice a day per nostril
Absorption
Following intranasal use, Azelastine hydrochloride has a systemic bioavailability of around 40% and reaches maximum concentration (Cmax) in 2-3 hours. In both Cmax and area under the curve (AUC), greater than proportional rise were seen when provided at dosages above the maximum dose suggested.
Volume of distribution
Azelastine's steady-state volume of distribution following intravenous and oral dosing is 14.5 L/kg.
Protein binding
Azelastine and desmethylazelastine had plasma protein binding of around 88% and 97%, respectively, according to in-vitro tests on human plasma.
Metabolism
The cytochrome P450 (CYP) enzyme system converts Azelastine hydrochloride into its primary and biologically active metabolite, desmethylazelastine. Although Azelastine labels mention that the specific CYP enzyme implicated has not been determined, it has been recommended that CYP3A4, CYP2D6, and CYP1A2 are principally responsible for the N-demethylation of Azelastine.
Route of elimination
Approximately 75% of radiolabeled Azelastine hydrochloride taken orally was eliminated in the stool, leaving fewer than 10% of the drug unaltered.
Half-life
Azelastine showed elimination half-life of 22 hours based on intravenous and oral dosing. Desmethylazelastine, its main active metabolite, exhibits elimination half-life of 54 hours.
Clearance
It showed a plasma clearance of 0.5 L/h/kg based on intravenous and oral dosing. [1]
None [5]
Central Nervous System Depressants: Depressants for central nervous system or alcohol should not be used concurrently with Azelastine. This is because these interactions may reduce alertness and influence central nervous system functioning. [5]
The most commonly noted side effects are:
Efficacy, Safety and Tolerability of Azelastine in patients with allergic rhinitis
In a meta-analysis of randomized controlled studies headed by Lee TA et al, Azelastine nasal spray was shown to be more effective than placebo in treating allergic rhinitis in terms of total symptom score. [6] Another study explored efficacy of Azelastine for treating symptoms of seasonal allergic rhinitis. Patients with seasonal allergic rhinitis participated in a 14-day, placebo-controlled, randomized, double-blind research. When compared to placebo, once-daily administration of Azelastine 0.15% nasal spray reduced a variety of nasal and ocular symptoms. [7]
Azelastine nasal spray is an effective monotherapy for people who still experience symptoms after receiving fexofenadine, and it should be taken into consideration in the initial management of patients with moderate-to-severe seasonal allergic rhinitis, according to a multicenter, randomized, double-blind, placebo-controlled, 2-week study. [8]
Another open-label study by Lieberman P et al. sought to examine Azelastine nasal spray's effectiveness to relieve symptoms of nonallergic vasomotor rhinitis, seasonal allergic rhinitis, and seasonal allergic rhinitis with nonallergic triggers (mixed rhinitis). Regardless of rhinitis diagnosis during the 2-week trial period, the second-generation antihistamine Azelastine aided to manage all rhinitis symptoms, including nasal congestion. [9]
A randomized, double-blind, parallel-group clinical investigation showed that 0.15% Azelastine nasal spray at 2 sprays/nostril twice a day was well-tolerated and remarkably reduced the nasal symptoms associated with seasonal allergic rhinitis. [10]
Azelastine vs. Desloratadine in people with allergen-induced seasonal allergic rhinitis
Azelastine nasal spray illustrated superior efficacy than Desloratadine tablets and placebo in a randomized, double-blind experiment carried out by Horak F et al. The decline in Total Nasal Symptom Score (TNSS) and Major Nasal Symptom Score (MNSS) was fastest following Azelastine therapy. For all nasal symptoms, including nasal congestion, Azelastine therapy resulted in a significant reduction in symptom severity. [11]
Azelastine vs. Mometasone furoate in seasonal allergic rhinitis patients
A research compared the onset of action and efficacy of Azelastine hydrochloride nasal spray to those of placebo and Mometasone furoate (an intranasal steroid) in individuals diagnosed with seasonal allergic rhinitis. Azelastine nasal spray demonstrated marked improvement in TNSS at 15 minutes when compared to placebo. Azelastine was found to be superior to both placebo and Mometasone nasal spray in minimizing nasal symptoms occurring within eight hours following allergen challenge. [12]













Comments (0)