Категории
Сменить пароль!
Сброс пароля!


Однако одним из главных вызовов современной гастроэнтерологии остаётся рост устойчивости H.pylori к антибиотикам. Во многих регионах мира резистентность штаммов превышает критические пороги, рекомендованные международными консенсусами (например, Maastricht V и Киотский глобальный консенсус), что существенно снижает эффективность стандартной эрадикационной терапии [4–7].
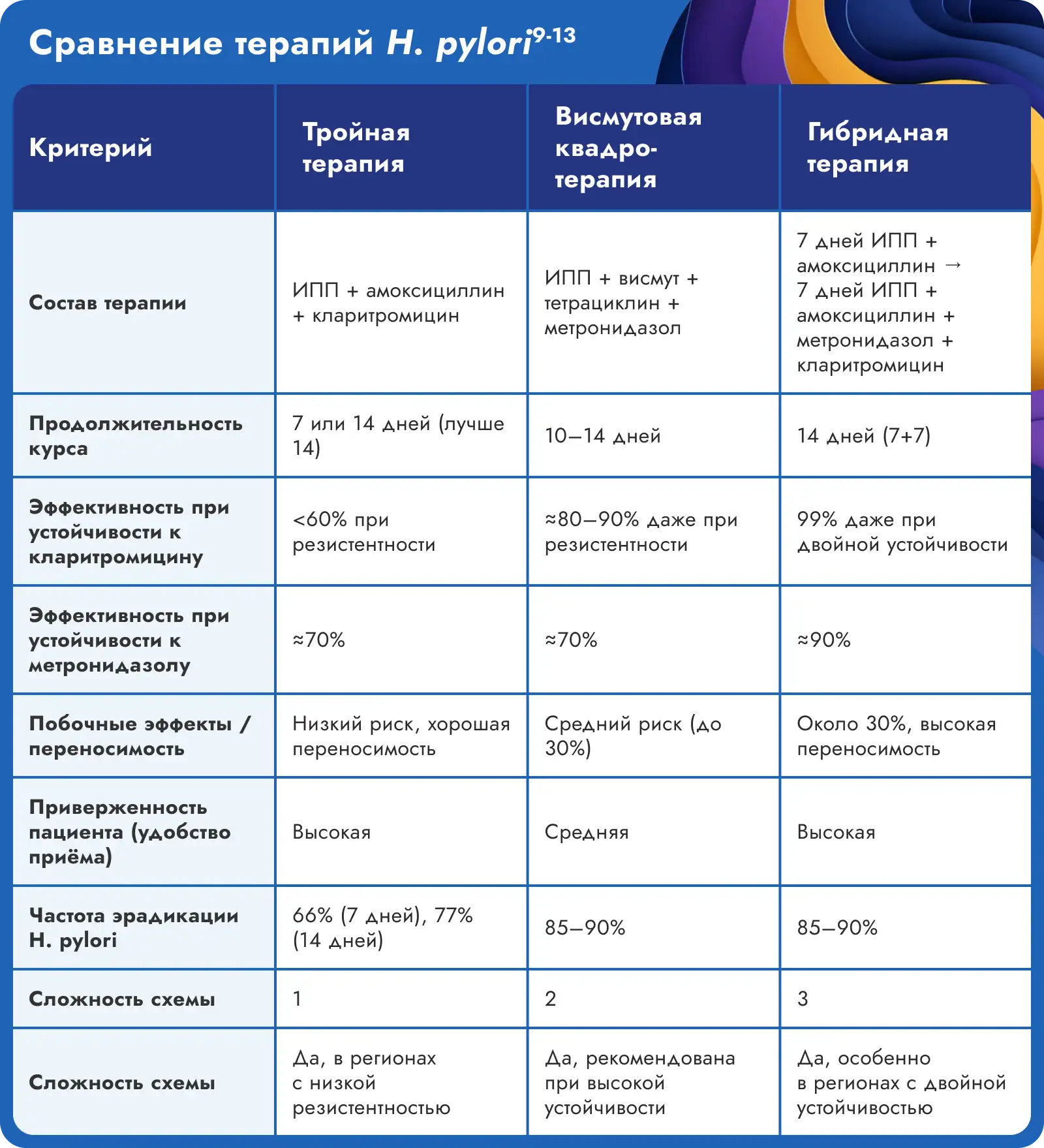
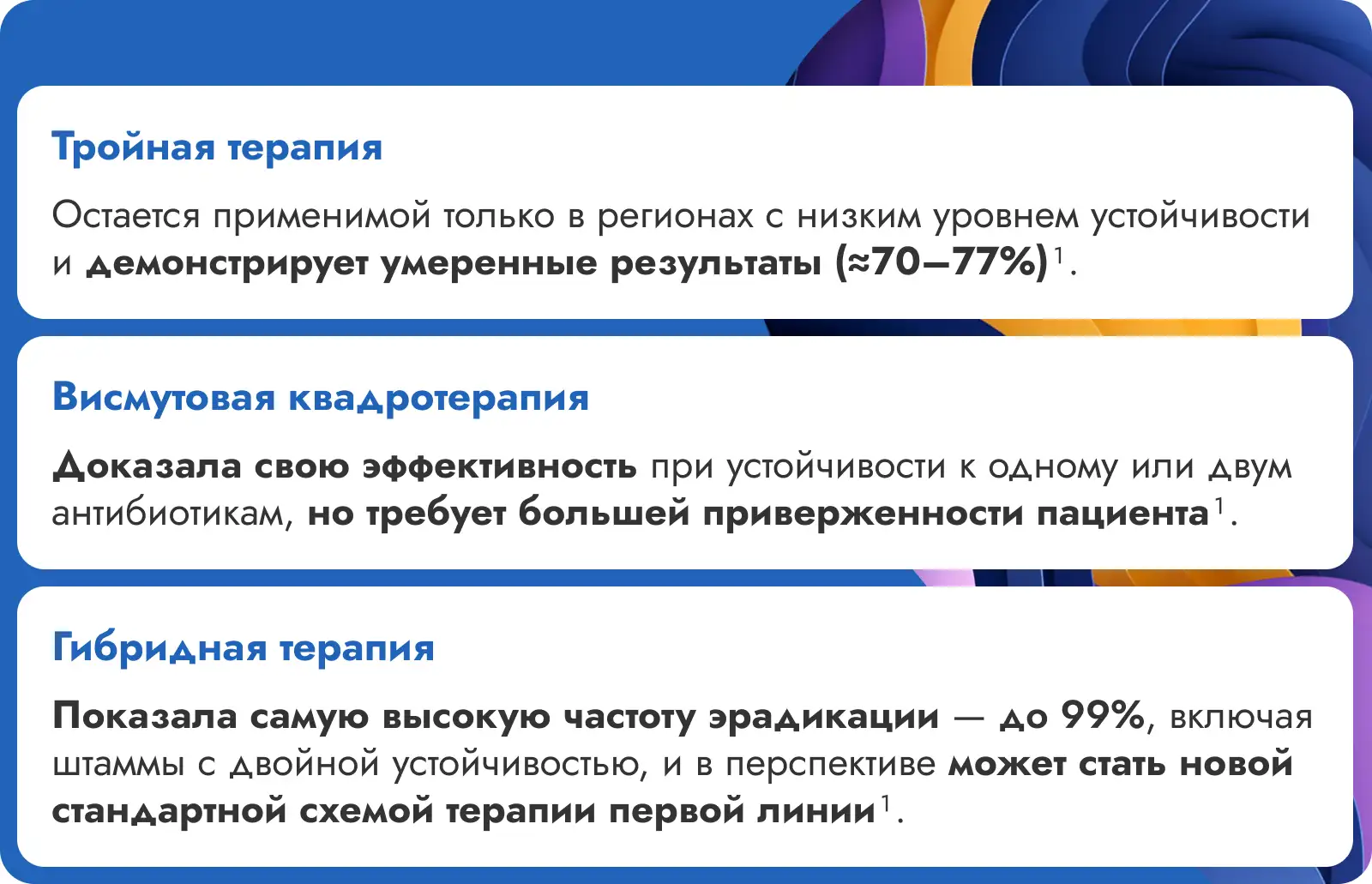
Из-за роста устойчивости Helicobacter pylori всё труднее подобрать терапию. Особенно это важно в регионах, где бактерия часто устойчива к кларитромицину. Поэтому всё чаще говорят о необходимости подбирать схему терапии индивидуально — с учётом особенностей конкретного пациента и антибиотикочувствительности. Для этого важно сравнить разные подходы к лечению: тройную терапию, висмутовую квадротерапию, а также гибридную схемы, чтобы выбрать наиболее подходящий вариант [5, 7, 8].
Исследования показывают, что схемы эрадикации H.pylori, включающие рабепразол, достигают высоких показателей успешности. Например, комбинация рабепразола с амоксициллином и кларитромицином в течение 7 дней продемонстрировала эффективность до 85% [14]. Также, четырехкомпонентная терапия с рабепразолом, висмутом, тетрациклином и метронидазолом показала успешность в 91,3% случаев [15].
Таким образом, включение рабепразола в схемы лечения H.pylori может способствовать повышению эффективности терапии, особенно в условиях растущей устойчивости бактерии к антибиотикам.


Источники:
1. Malfertheiner P., Megraud F., O’Morain C.A., et al. Management of Helicobacter pylori infection—the Maastricht IV/Florence Consensus Report. Gut. 2012;61(5):646–664.
2. Dinis-Ribeiro M., Areia M., de Vries A.C., et al. Management of precancerous conditions and lesions in the stomach (MAPS): guideline from the European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter Study Group (EHSG), European Society of Pathology (ESP), and the Sociedade Portuguesa. Endoscopy. 2012;44(1):74–94.
3. Banic M., Franceschi F., Babic Z., Gasbarrini A. Extragastric manifestations of Helicobacter pylori infection. Helicobacter. 2012;17 Suppl 1:49–55.
4. Chen B-F., Xu X., Deng Y., et al. Relationship between Helicobacter pylori infection and serum interleukin-18 in patients with carotid atherosclerosis. Helicobacter. 2013;18(2):124–128.
5. Megraud F., Coenen S., Versporten A., et al. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut. 2013;62(1):34–42.
6. Selgrad M., Malfertheiner P. Treatment of Helicobacter pylori. Curr Opin Gastroenterol. 2011;27(6):565–570.
7. Sugano K., Tack J., Kuipers E.J., et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015;64(9):1353–1367.
8. McNulty C.A.M., Lasseter G., Shaw I., et al. Is Helicobacter pylori antibiotic resistance surveillance needed and how can it be delivered? Aliment Pharmacol Ther. 2012;35(11):1221–1230.
9. Ахметова Д.Г., Балтабекова А.Ж., Шустов А.В. Устойчивость к антибиотикам Helicobacter pylori: обзор эпидемиологических тенденций и проблемы терапии // РМЖ. Медицинское обозрение. – 2018. – № 7(I). – С. 13–18. – URL: https://www.rmj.ru/articles/gastroenterologiya/Ustoychivosty_k_antibiotikam_Helicobacter_pylori_obzor_epidemiologicheskih_tendenciy_i_problemy_terapii/ (дата обращения: 27.05.2025).
10. Maastricht V/Florence Consensus Report. Management of Helicobacter pylori infection—the Maastricht V/Florence Consensus Report // Gut. 2017. Vol. 66. P. 6–30. DOI: 10.1136/gutjnl-2016-312288.
11. Georgopoulos S.D., Papastergiou V., Martinez-Gonzalez B. et al. Hybrid therapy as first-line regimen for Helicobacter pylori eradication in a high clarithromycin resistance area: a prospective open-label trial // Annals of Gastroenterology. 2018. Vol. 31(2). P. 205–210. DOI: 10.20524/aog.2017.0221.
12. Paoluzi O.A., Andrei F., Papa A. et al. Efficacy of 7-day versus 14-day triple therapy for the eradication of Helicobacter pylori: a prospective study // Digestive and Liver Disease. 2004. Vol. 36(8). P. 511–515. DOI: 10.1016/j.dld.2004.03.002.
13. Chey W.D., Leontiadis G.I., Howden C.W., Moss S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection // Am. J. Gastroenterol. 2017. Vol. 112(2). P. 212–238. DOI: 10.1038/ajg.2016.563.
14. Gisbert JP, Khorrami S, Calvet X, Pajares JM. Systematic review: Rabeprazole-based therapies in Helicobacter pylori eradication. Aliment Pharmacol Ther. 2003 Mar 15;17(6):751-64. doi: 10.1046/j.1365-2036.2003.01450.x. PMID: 12641497.
15. Nguyen, L.T.; Nguyen, V.B.; Tran, T.V.; Duong, H.Q.; Le, L.T.T.; Phuong, M.H.T.; Nguyen, T. Efficacy of Helicobacter pylori Eradication Based on Rabeprazole–Bismuth–Tetracycline–Tinidazole Regimen in Vietnamese Patients with Duodenal Ulcers. Gastroenterol. Insights 2022, 13, 365-376. https://doi.org/10.3390/gastroent13040036
R1355902-02062025-HCP















Комментарии (0)