Categories
Change Password!
Reset Password!



Intranasal saline offers symptom relief similar to intranasal steroids in pediatric obstructive sleep-disordered breathing, with no additional benefit from corticosteroid therapy.
In childhood, symptoms of obstructive sleep apnea are common and are linked with comorbidity. While adenotonsillectomy remains the standard first-line treatment, non-surgical therapies are increasingly explored to alleviate symptom burden and avoid or delay surgery. Hence, this study explored the potency of 6 weeks of intranasal saline compared with intranasal steroid (INS) in kids suffering from obstructive sleep-disordered breathing (OSDB).
In this double-blind, randomized clinical trial, 150 kids (aged 3-12 years) were incorporated. All the kids first underwent a 6-week run-in phase using once-daily intranasal saline. Those with persistent symptoms, defined as a sleep-disordered breathing (SDB) score ≥ −1, were then randomly divided to receive either once-daily intranasal mometasone furoate at a dose of 50 micrograms or continued saline for an additional 6 weeks.
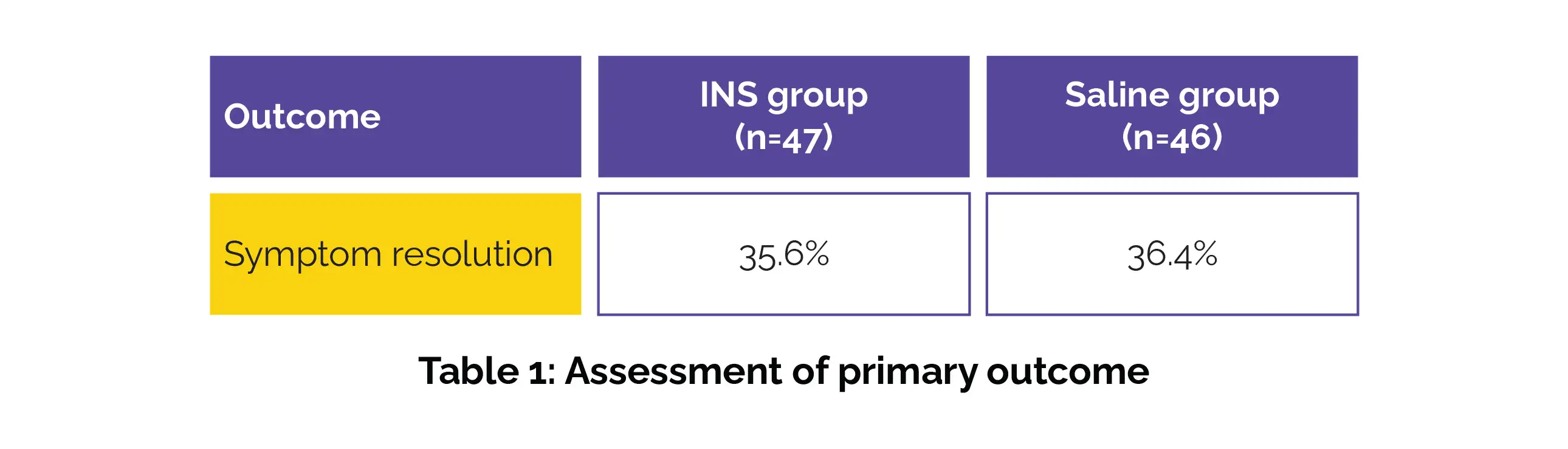
In total, 93 kids were male, accounting for 62%. Of the 139 kids who completed the run-in phase, 41 kids, or 29.5%, attained symptom improvement after saline alone. Similar symptom resolution was observed in the INS group (35.6%) and the saline group (36.4%), showing no significant difference (risk difference −0.9%), as depicted in Table 1:
Secondary outcomes—including quality of life, behavior, and parental perception of surgical need—were also similar. Subgroup analyses did not identify any population that benefited more from steroid therapy.
Overall, approximately one-third of children improved with initial saline therapy alone, and a similar proportion attained symptom resolution during the second phase regardless of treatment allocation, resulting in a cumulative resolution rate of around 50%. These findings suggest that INS is an effective, low-cost, and well-tolerated first-line option for pediatric OSDB. The lack of added benefit with INS supports a conservative management approach before considering sleep studies or surgical interventions such as adenotonsillectomy.
JAMA Pediatrics
Intranasal Treatments for Children With Sleep-Disordered Breathing: The MIST+ Randomized Clinical Trial
Gillian M Nixon et al.












Comments (0)