Categories
Change Password!
Reset Password!


Tradipitant is a centrally acting antiemetic approved by the Food and Drug Administration (FDA) on 30 December 2025 for the prevention of motion sickness–related vomiting in adults.
Tradipitant is a centrally acting antiemetic approved by the Food and Drug Administration (FDA) on 30 December 2025 for the prevention of motion sickness–related vomiting in adults.[1,2] Unlike traditional antihistamines or anticholinergics, tradipitant targets substance P-mediated pathways, offering a novel mechanism for managing emesis.[3]
Pharmacological Class: Neurokinin-1 (NK1) receptor antagonist
It prevents vomiting induced by motion sickness in adults.[4]
The NK1 receptor is a G protein–coupled receptor that primarily interacts with substance P, a neuropeptide released by both nerve cells and inflammatory cells.[2] Tradipitant selectively blocks NK1 receptors, with negligible binding affinity for other receptor systems, including:
By blocking the action of substance P at these receptors, it prevents the transmission of nausea and vomiting signals from both central and peripheral pathways.[6]
Absorption
Distribution
Metabolism
It is extensively metabolized and involves both CYP-dependent and non-CYP pathways:
Elimination
None
Strong CYP3A4 inhibitors: Tradipitant is metabolized by CYP3A4. Hence, concomitant use with strong CYP3A4 inhibitors may increase systemic exposure, potentially leading to a heightened risk of adverse effects.[4]
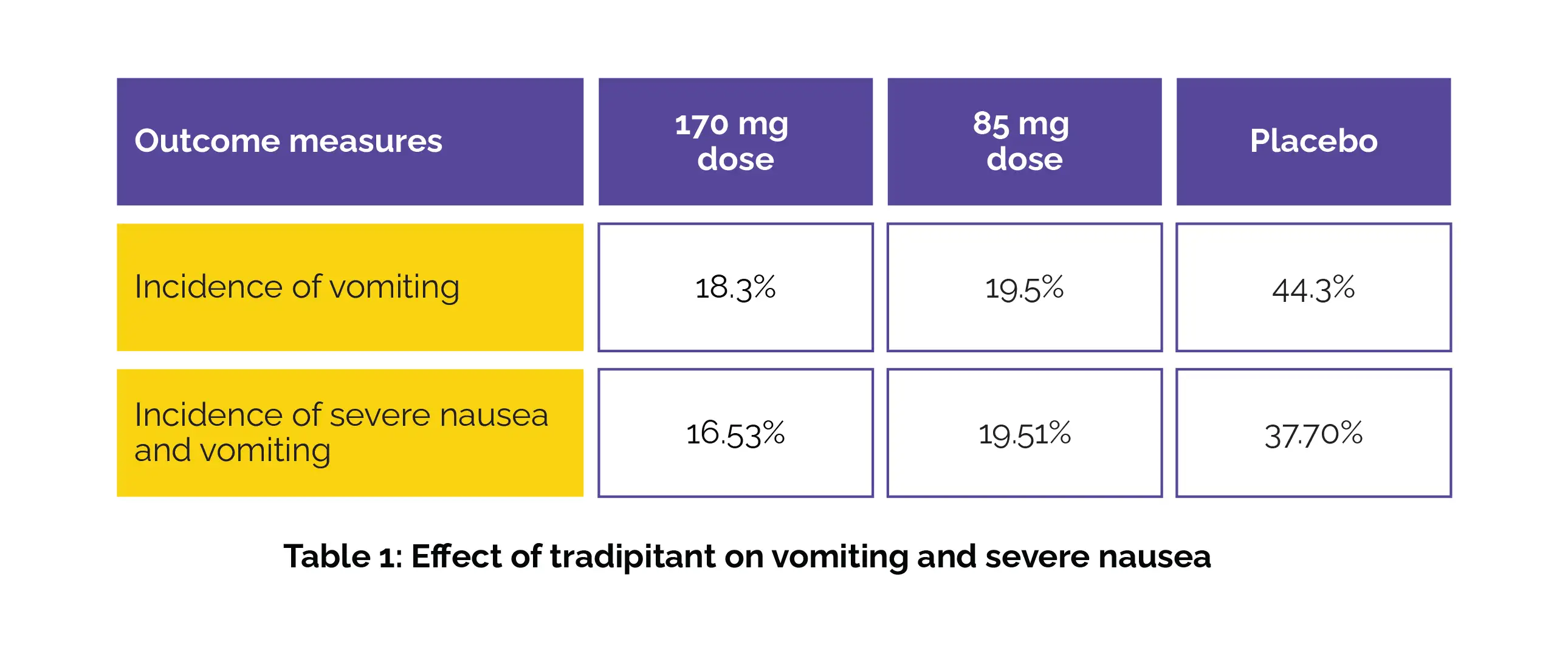
1. Motion SYROS Trial
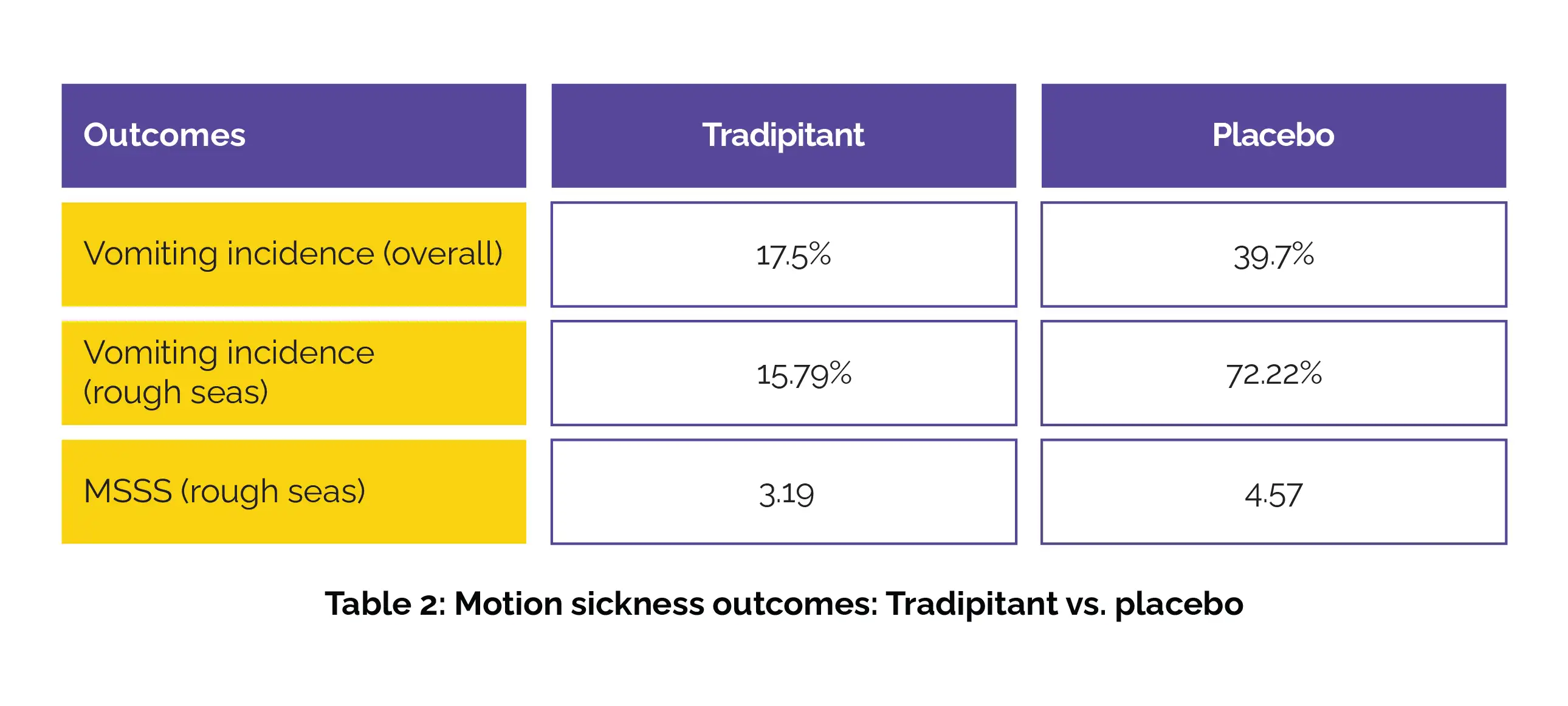
2. Motion SIFNOS Trial










Comments (0)