Categories
Change Password!
Reset Password!


Semaglutide, a Food and Drug Administration (FDA)-approved long-acting glucagon-like peptide-1 (GLP-1) receptor agonist, has transformed the management of type 2 diabetes mellitus (T2DM) and obesity.
Semaglutide, a Food and Drug Administration (FDA)-approved long-acting glucagon-like peptide-1 (GLP-1) receptor agonist, has transformed the management of type 2 diabetes mellitus (T2DM) and obesity. By mimicking the natural incretin hormone GLP-1, it improves metabolic control through multiple glucose-regulating mechanisms.[1,2]
Pharmacological class: GLP-1 receptor agonist
It is indicated:
1. As an add-on to lifestyle modification (exercise and diet) for improving glycemic control in adults with T2DM.[3]
2. As an add-on to decreased calorie diet and elevated physical activity for chronic weight management in:
(a) Adults with an initial body mass index (BMI) ≥30 kg/m² (obesity), or BMI ≥27 kg/m² (overweight) when a minimum of one weight-related condition is present, such as hypertension, T2DM, or dyslipidemia.
(b) Adolescents aged 12 years and above with an initial BMI at or above the 95th percentile for age and sex, consistent with obesity.[4]
3. For adults with established cardiovascular (CV) disease and overweight or obesity to lower the likelihood of major adverse cardiovascular events (MACE), including non-fatal stroke, CV death, and non-fatal myocardial infarction/heart attack.
4. For adults with T2DM and chronic kidney disease to decrease the likelihood of sustained drop in estimated glomerular filtration rate (eGFR), transition to end-stage renal disease, and CV death.
5. For adults with established CV disease and a BMI ≥27 kg/m² to reduce the chances of heart attack (non-fatal myocardial infarction).
Note: Semaglutide has also received accelerated approval from the FDA in August 2025 for the treatment of adults with metabolic-associated steatohepatitis (MASH) and moderate-to-advanced liver fibrosis.[5]
1. Mechanism of glycemic control
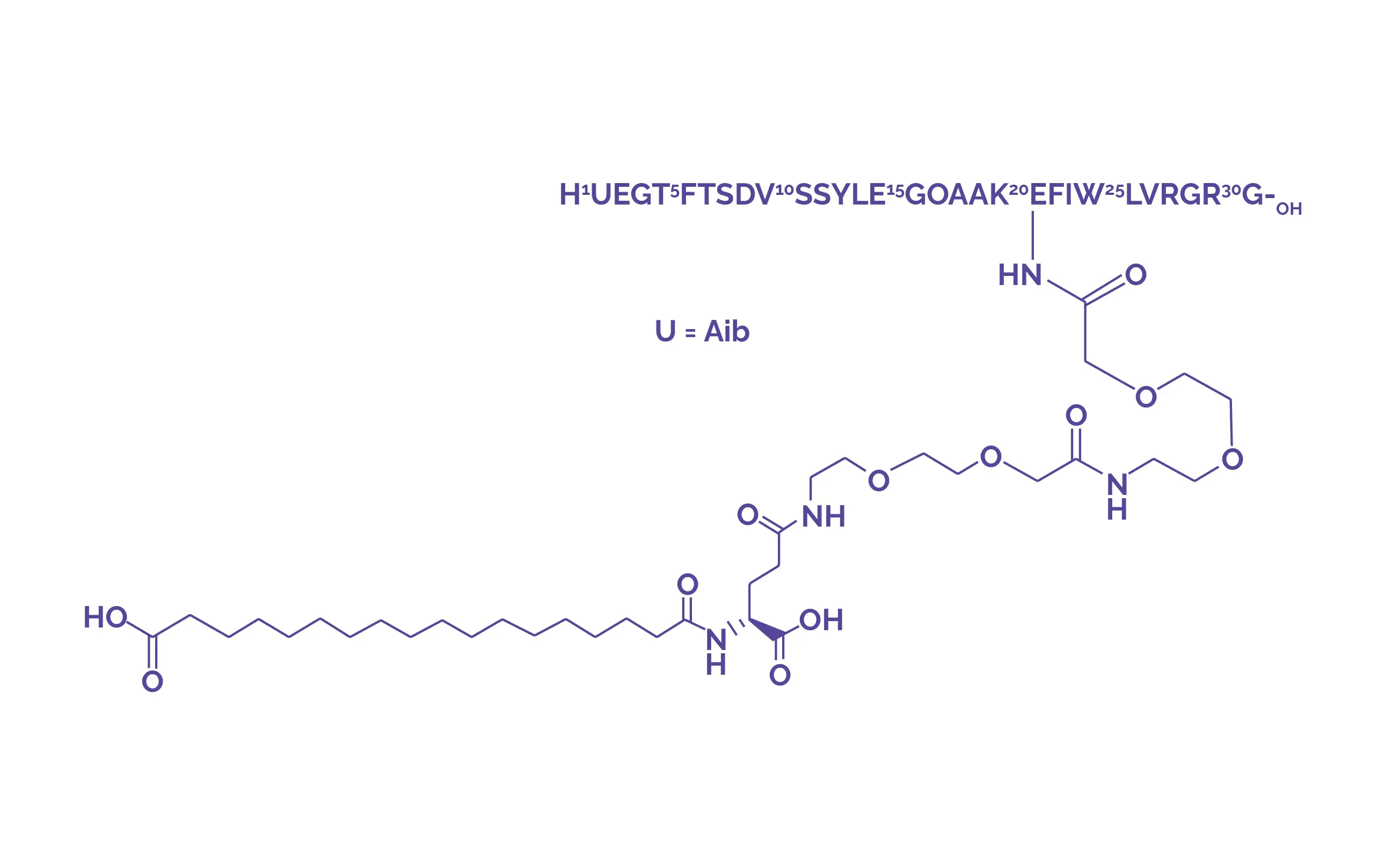
GLP-1, a natural hormone, plays a fundamental role in governing blood glucose levels. It improves glycemic control by slowing gastric emptying, improving insulin secretion, and minimizing glucagon release after meals. Normal glucose balance also depends on pancreatic beta-cell hormones such as insulin and amylin.
Semaglutide, a GLP-1 receptor agonist that shares about 94% structural similarity with human GLP-1, mimics this physiological hormone. It selectively binds to GLP-1 receptors on pancreatic islet cells, enhancing insulin synthesis and suppressing glucagon secretion. These effects occur in a glucose-dependent way, helping lower blood glucose while diminishing the risk of excessive hypoglycemia.
2. Mechanism of CV benefit and weight loss
Beyond glycemic control, semaglutide may contribute to CV protection. In conditions such as hypercholesterolemia, it is thought to slow the progression of atherosclerosis by decreasing intestinal permeability and inflammatory processes. The medication also promotes weight loss primarily by diminishing appetite and food cravings, resulting in lower calorie intake.[5]
1. For T2DM and CV disease
2. For chronic weight management
Absorption
Distribution
Metabolism
Elimination
Semaglutide is contraindicated in:
1. Evidence from the STEP 1 trial
In a double-blind trial involving 1961 adults with obesity or overweight without diabetes, once-weekly semaglutide 2.4 mg combined with lifestyle intervention produced substantially greater weight loss than placebo over 68 weeks. Mean body weight decreased by 14.9% with semaglutide versus 2.4% with placebo, corresponding to a treatment difference of −12.4 percentage points. In absolute terms, participants receiving semaglutide lost 15.3 kg compared with 2.6 kg in the placebo group.
Clinically meaningful weight reduction was achieved by a remarkably higher proportion of participants treated with semaglutide: 86.4% lost ≥5% of body weight, 69.1% lost ≥10%, and 50.5% lost ≥15%, compared with 31.5%, 12.0%, and 4.9% in the placebo group, respectively. Treatment with semaglutide also resulted in better improvements in physical functioning and cardiometabolic risk determinants.[6]
2. Evidence from the STEP 2 trial
The STEP 2 trial investigated once-weekly semaglutide 2.4 mg for weight control in adults with overweight or obesity and T2DM. After 68 weeks of treatment, participants receiving semaglutide 2.4 mg experienced a mean body weight reduction of 9.6%, compared with 3.4% with placebo, corresponding to a −6.2 percentage-point treatment difference. A substantially greater proportion of participants treated with semaglutide 2.4 mg achieved ≥5% weight loss than those receiving placebo (68.8% vs 28.5%).[7]
3. Evidence from the STEP 4 trial
In a 68-week randomized withdrawal trial involving adults with obesity or overweight without T2D, continued treatment with semaglutide 2.4 mg once weekly markedly improved long-term weight-loss maintenance. Following a 20-week run-in phase, participants achieved a mean weight reduction of 10.6% before randomization.
Over the subsequent 48 weeks, participants who continued semaglutide experienced an additional mean weight loss of 7.9%, whereas those switched to placebo regained 6.9% of body weight, resulting in a significant −14.8 percentage-point treatment difference. Continued semaglutide therapy also produced greater reductions in waist circumference (−9.7 cm) and systolic blood pressure (−3.9 mm Hg) and improved physical functioning scores when compared with placebo.[8]
4. Evidence from SUSTAIN trials
Across multiple phase 3 trials (SUSTAIN 1–6 and additional studies), semaglutide consistently produced greater reductions in glycated hemoglobin (HbA1c; up to 1.8%) and body weight compared with placebo and several active treatments, including sitagliptin, exenatide (extended-release), dulaglutide, and insulin glargine.In the SUSTAIN 6 trial, semaglutide also demonstrated CV safety and significantly reduced MACE compared with placebo, confirming its noninferiority while suggesting potential CV protection.[9]
5. Pooled evidence from SOUL, SUSTAIN-6, and PIONEER-6 trials
A systematic review and meta-analysis explored the CV effects of semaglutide in patients with T2DM. Three trials—SOUL Trial, SUSTAIN-6 Trial, and PIONEER-6 Trial—including 16,130 participants were analyzed. The pooled results showed that semaglutide reduced MACE—CV death, nonfatal myocardial infarction, and nonfatal stroke—with a hazard ratio of 0.83, representing a 17% relative risk reduction and low heterogeneity (I² = 25%). Adverse events were comparable between the semaglutide and placebo groups. Overall, semaglutide remarkably lowers CV risk in T2DM, supporting its use for both glycemic control and CV risk reduction.[10]
1. Pawar SS, Rasal PB, Kulkarni KH, Pawar SB. Semaglutide: A Comprehensive Review of its Pharmacology, Clinical Applications, and Future Therapeutic Potential. Journal of Drug Delivery & Therapeutics. 2025 Dec 1;15(12).
2. Kommu S, Whitfield P. Semaglutide. [Updated 2024 Feb 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603723/. Bookshelf ID: NBK603723, PMID: 38753931.
3. OZEMPIC (semaglutide) injection. FDA label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/209637lbl.pdf
4. WEGOVY (semaglutide) injection. FDA label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215256s007lbl.pdf
5. Semaglutide. Drug Bank [DB13928]. Available from:
https://go.drugbank.com/drugs/DB13928
6. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I. Once-Weekly Semaglutide in Adults with Overweight or Obesity. The New England Journal of Medicine. 2021 Mar 18;384(11):989-1002.
7. Davies M, Færch L, Jeppesen OK, Pakseresht A, Pedersen SD, Perreault L et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021 Mar 13;397(10278):971-984.
8. Rubino D, Abrahamsson N, Davies M, Hesse D, Greenway FL, Jensen C et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021 Apr 13;325(14):1414-1425.
9. Goldenberg RM, Steen O. Semaglutide: Review and Place in Therapy for Adults With Type 2 Diabetes. Canadian Journal of Diabetes. 2019 Mar;43(2):136-145.
10. Adinolfi G, Milia V, Dinkov B, Stavreva G. Cardiovascular Outcomes Associated with Semaglutide in Type 2 Diabetes: A Systematic Review and Meta-Analysis. Endocrines. 2026 Mar 4;7(1):9.













Comments (0)